
Anterior mediastinal mass lesions
On frontal chest X-Ray
Introduction
Recognising the appearance of an anterior mediastinal mass on chest X-Ray is a key skill in radiology as these lesions are much less often caused by primary lung cancers changing the differential.
In this article, we will explore a case of a young adult presenting with an anterior mediastinal mass.
We’ll walk through the key imaging features, the diagnostic reasoning process, and how to use simple signs like the hilum overlay sign to localise and narrow the differential.
Case introduction
A female in her 30s presents with chest pain and has a chest X-Ray through her GP. Can you see anything that might help you localise the abnormality?
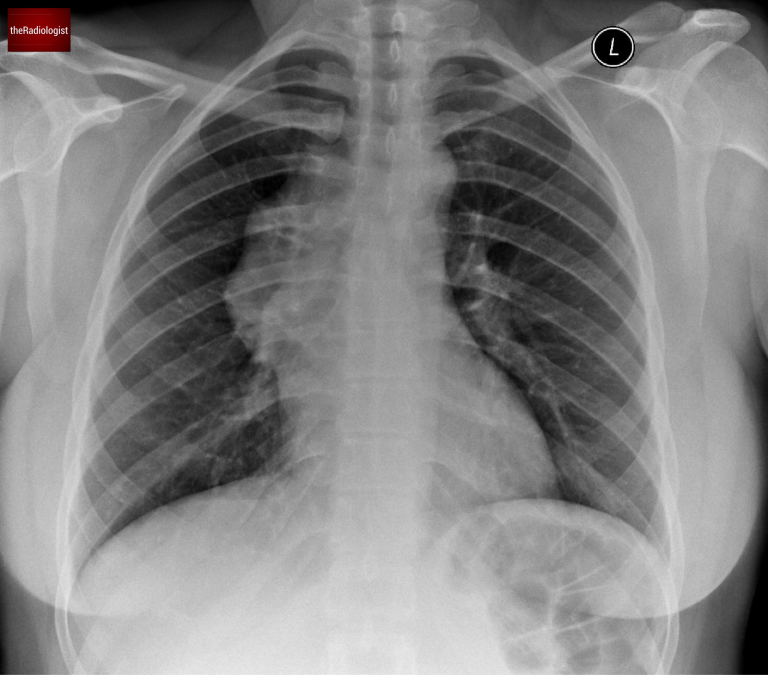
PA view of a chest X-Ray of a female in her 30s
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Mediastinal findings
To get oriented, let’s start with a comparison and compare our case with a normal X-Ray.
Normal Anatomy
In a normal X-ray, we should be able to see the faint outline of the brachiocephalic veins draining into the superior vena cava (SVC) on the right side of the mediastinum.
You can also see a small contour representing the azygos vein just above the right main bronchus.
Our Case
In this case, those normal contours are missing. Instead, we see an abnormal contour along the right side of the mediastinum.
Could this be lung cancer? It’s a fair question, but there’s a key sign that points us away from lung cancer and towards other differentials.
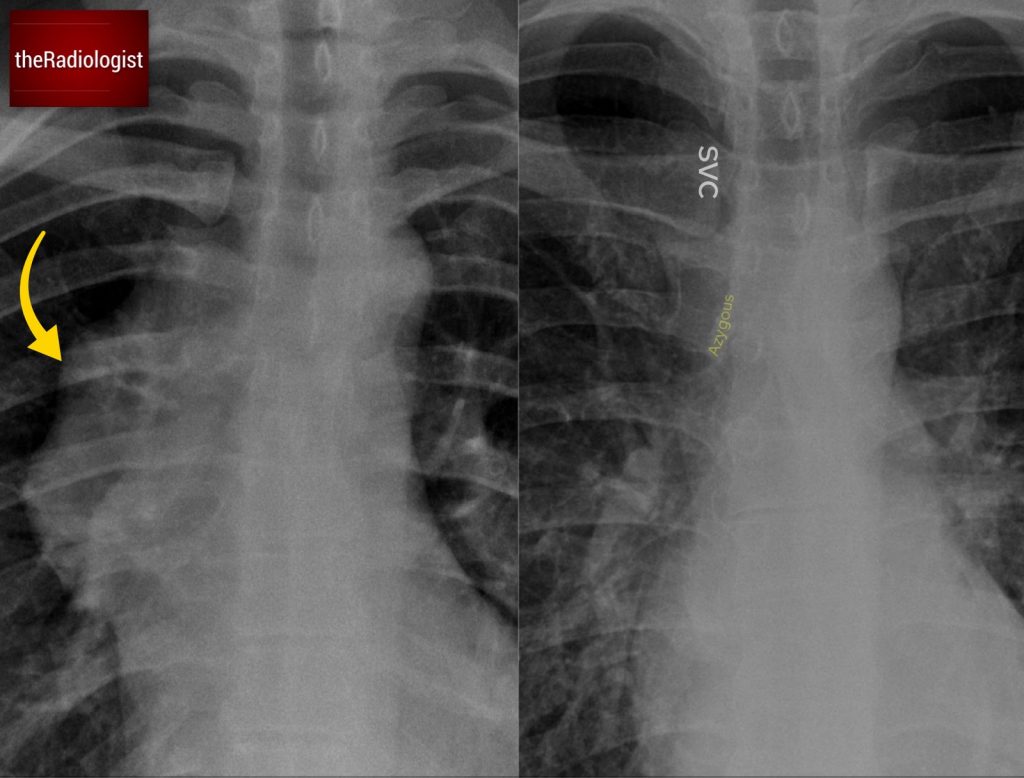
Compare the normal anatomy (right) with our case (left). In normal circumstances we should be able to see a faint opacity reflecting the SVC and brachiocephalic veins as well as an azygos contour. In our case these are more difficult to spot with an abnormal contour to the right side of the mediastinum.
Hilum overlay sign
Take a closer look at the X-ray. Through the abnormal mass, you can still make out the right hilar vessels. This tells us something crucial:
- If the mass were in the middle mediastinum, we wouldn’t be able to see the hilum because it would obscure those structures.
- This phenomenon is called the hilum overlay sign.
Most central lung cancers are located in the middle mediastinum or involve the hilar region, and although there handful of occasions where I have seen lung cancers present with a hilum overlay sign on X-Ray, it makes lung cancer much less likely. Instead, we need to consider a mass in either the anterior or posterior mediastinum.
Statistically, anterior mediastinal masses are the most common culprits in cases with a hilum overlay sign although there are times where it can be caused by a posterior mediastinal lesion. Make sure you look for signs of a posterior mediastinal lesion such as loss of the contour of the descending aorta or an abnormality of a paraspinal line: in this case these features of a posterior mediastinal lesion are absent.
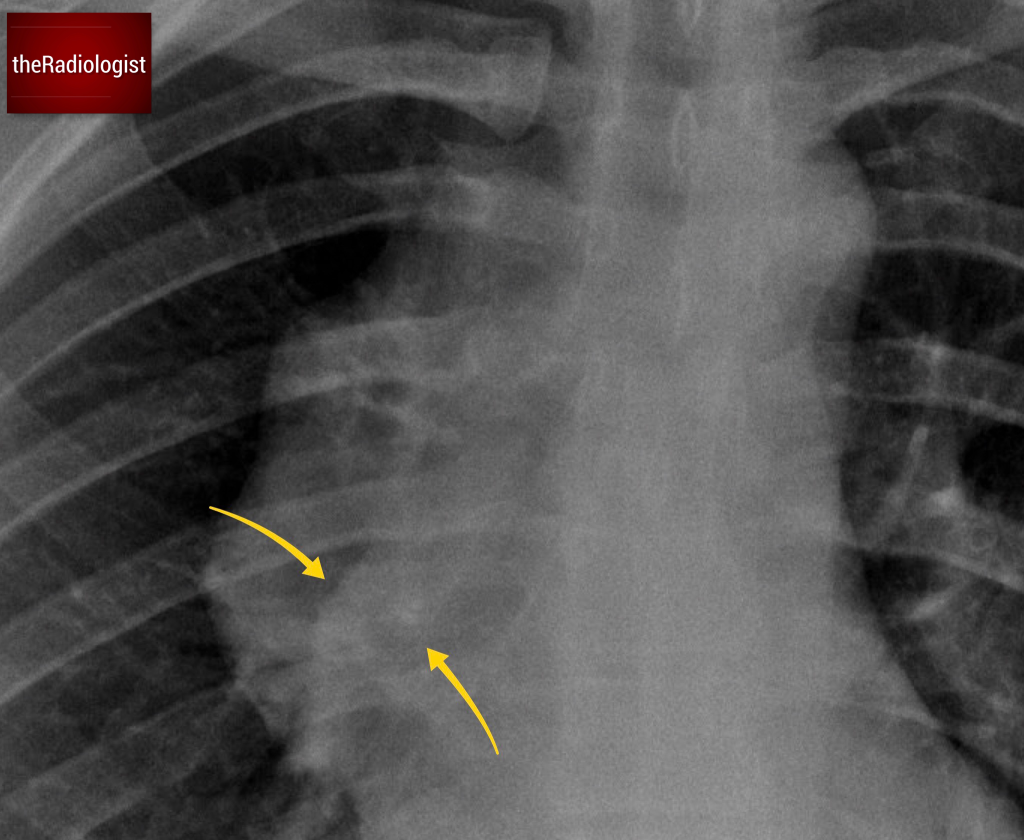
Look through the mass and you will see the right hilar vessels: if you can see the vessels through a hilar mass (yellow arrow) this is called the hilum overlay sign and points you away from a middle mediastinal lesion.
Anterior mediastinal mass differential
So, what could cause an anterior mediastinal mass? Let’s use the 4 T’s mnemonic:
- Thymic lesions
- Teratomas or other germ cell tumors
- Thyroid goiter
- ‘Terrible’ lymphoma
Here’s an important age-related tip:
- In patients under 40, germ cell tumors and lymphoma are more common.
- Over 40, thymomas are more common.
KEY POINT
A single well defined anterior mediastinal lesion in a patient over the age of 50 is most likely to represent a thymoma and can commonly be resected without need for biopsy.
Workup
The CT scan here shows a clear mass in the anterior mediastinum, while the hilum remains untouched. This finding explains the hilum overlay sign we observed on the X-ray.
CT imaging can also help differentiate between the causes of anterior mediastinal masses:
- Calcification: Seen in germ cell tumors or thymomas.
- Fat within the lesion: Points toward a teratoma.
- Thyroid connection: Look for continuity with the thyroid gland and similar enhancement patterns.
- Pleural or pericardial involvement: A hallmark of thymic lesions.

CT confirms a mass within the anterior mediastinum.
To confirm the nature of this mass, firstly a FDG PET-CT scan was performed showing intense avidity within the lesion and a small number of small lymph nodes within the medistinum, pointing towards lymphoma.
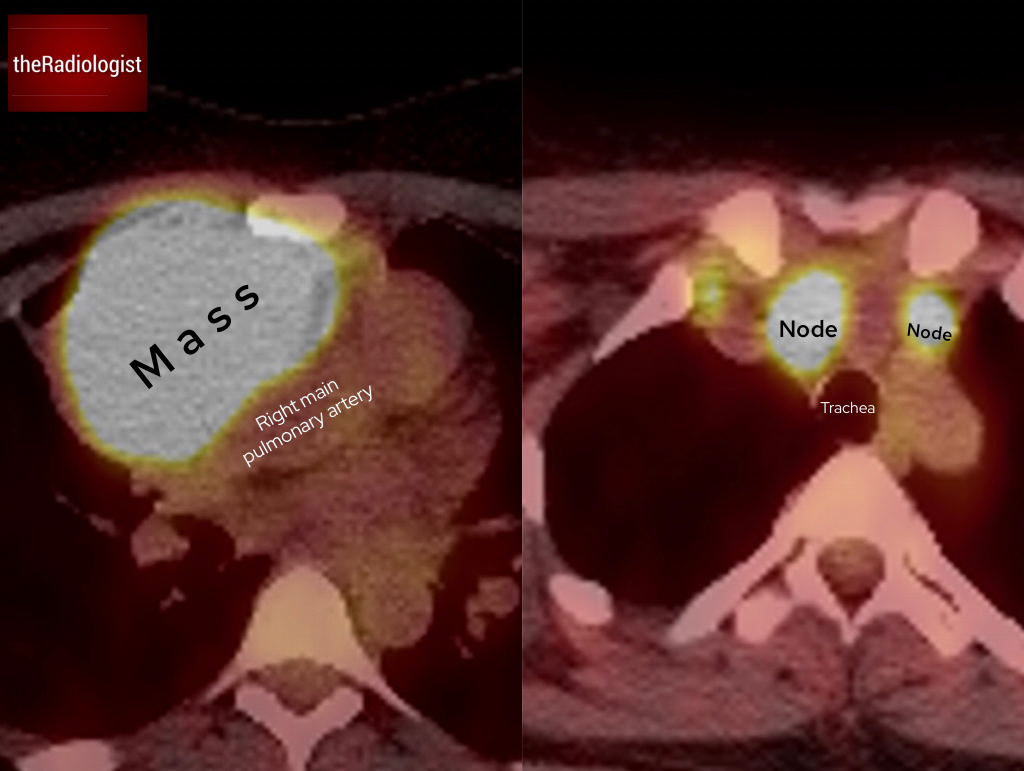
FDG PET-CT shows intense avidity within the lesion and a small number of lymph nodes within the mediastinum.
A CT-guided biopsy was performed through an anterior approach. This confirmed a diagnosis of B-cell lymphoma.

CT guided biopsy of the anterior mediastinal lesion confirmed a diagnosis of B-cell lymphoma.
Follow-up
Follow up for lymphoma usually involves a PET-CT however have a look at the post chemotherapy X-Ray. This shows that the mass has completely resolved.

The follow -up chest X-Ray after chemotherapy shows resolution of the anterior mediastinal mass and now a normal contour on the right side of the mediastinum.
KEY POINT
Whenever you see an abnormal mediastinal contour on a chest X-ray, remember to look for the hilum overlay sign.
It’s a small detail, but it makes a big difference in narrowing down your diagnosis.