Assessing a CT KUB is a key skill for anyone performing emergency work in a hospital. In this case we will go through how to systematically assess a CT KUB for obstructing calculi and so by the end of the article you should be able to look for hydronephrosis and these obstructing calculi.
A male in his 30s presents with abdominal pain. Here is a non contrast CT of his abdomen and pelvis.
I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
CT KUB
Here we have a CT KUB, a commonly performed study in Emergency Departments all around the world looking for renal calculi and its consequences.
A lot of departments perform these with the patient on their front (prone rather than supine): this helps in cases where it is hard to differentiate whether a calculus lies within the bladder or the vesico-ureteric junction (VUJ). In cases where the stone lies in the bladder the calculus will fall and be seen in a dependent position, unlike a VUJ stone.
These scans are done without contrast as the presence of bright contrast could mask stones which usually look bright on a non contrast CT.
Initial assessment
In this case the left renal pelvis is dilated, ie there is hydronephrosis. As soon as you see this in the context of renal colic it is pretty likely there is an obstructing stone, however remember there are other causes of obstruction eg intrinsic tumour (TCC), lymph nodes compressing the ureter and clot. In any CT KUB it is important to follow the renal pelvis down to the ureter, see if this is dilated in addition, then try and track its course in front of the psoas muscle into the pelvis.
First identify the renal pelvis then follow it down to the ureter to see if you can find the source of obstruction.
Dilated pelvis only?
In some cases you may just find a dilated renal pelvis without a dilated ureter and without a stone. Check to see if the calyces are dilaed – if they aren’t you could just be dealing with an ‘extra-renal pelvis’ which is a variant. If the calyces are dilated then you have pelvi-ureteric junction obstruction (PUJ obstruction). The cause for this can be idiopathic and in some cases can be due to a crossing vessel. Thinning of the cortex can be a clue it has been going on for some time. A post contrast CT urogram is usually a good idea in these cases to exclude an obstructing pelvic tumour.
Follow the ureter
In this case when we follow the ureter to its distal third we find a bright calculus which accounts for the obstruction.
Sometimes calcified phleboliths which lie in blood vessels can cause confusion and can be mistaken for calculi – this is why it is really important to familiarise yourself with the normal course of the ureter which usually pass in front of the psoas and insert posteriorly into the bladder. It can be really useful to have a previous scan to compare to and confirm you have unchanged phleboliths. If there is any doubt you can consider a post contrast CT urogram where you opacify the ureters (delayed phase) to ensure the calcified foci do not lie within the ureter.
In this case we can find an obstructing calculus.
KEY POINTS
Be methodical in following the ureter in any CT KUB study: hydronephrosis and perinephric stranding should alert you to a possible obstructing stone.
Compare to previous scans if you find what could be calcified pelvic phleboliths. A post contrast CT urogram can be used as a problem solving tool if you aren’t sure.
FREE GUIDE
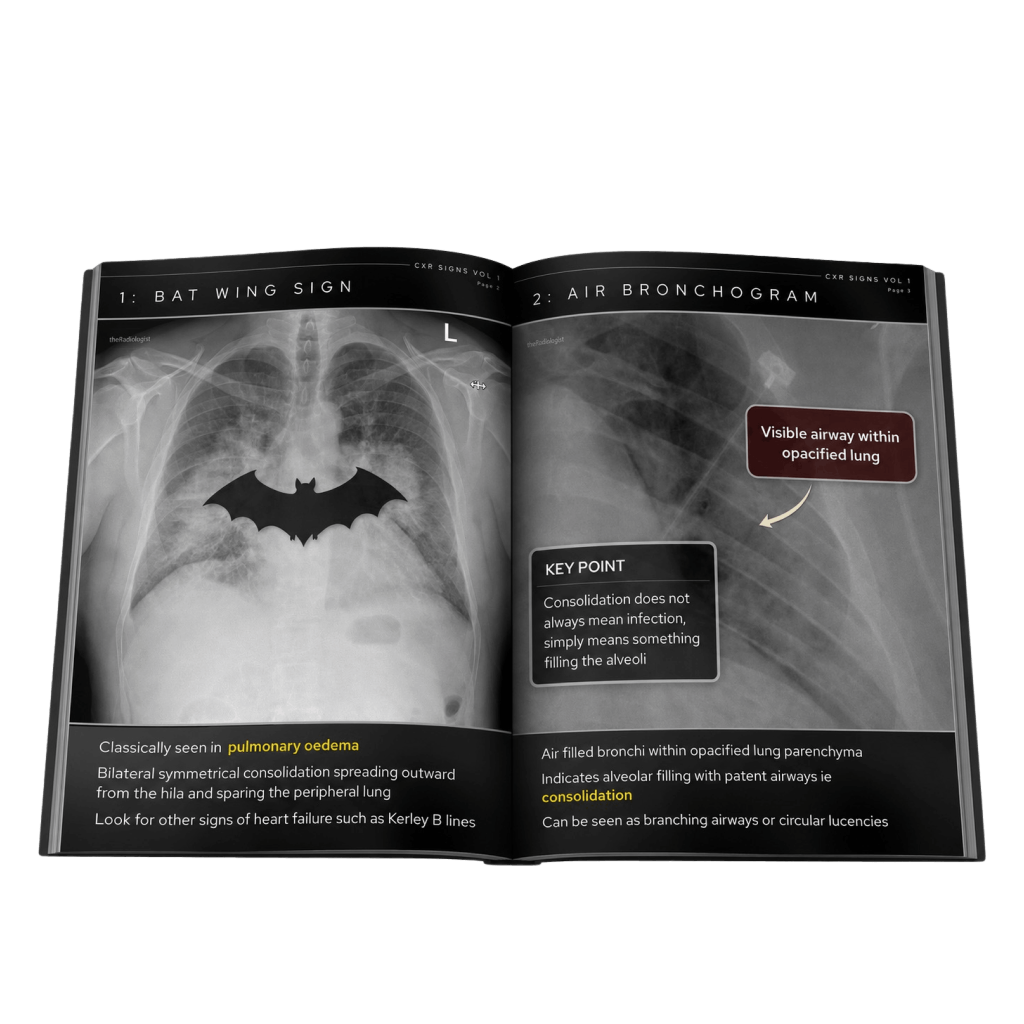
Free guide: 20 Chest X-Ray signs you need to recognise
Downloaded by 10,000+ healthcare professionals. Get 20 annotated chest X-ray signs with clear teaching points and explanations. Written by a Consultant Radiologist, this free guide is designed to help you recognise important findings more confidently when reviewing chest X-Rays.
You’ve got the framework now let’s put it to work. Dive into a related case to see these findings on real images, or explore another guide to build out your systematic approach. That’s where it really starts to stick.