Small bowel tumours
CT features, causes and differential diagnosis
Introduction
A 60-year-old man presents with months of abdominal pain, and a contrast-enhanced CT reveals more than one area of concern.
We’ll walk through the key imaging features, discuss the differential for small bowel mural thickening, and explore how findings in the stomach and bowel can point toward a unifying diagnosis.
Case introduction
A 60-year-old male presents with a few months of abdominal pain. A post-contrast CT scan of the abdomen and pelvis in a portovenous phase shows some abnormalities. Let’s go through the case.
Have a look at the scan below. I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Case findings
There are two areas on the scan in particular that appear abnormal: the stomach and the small bowel.
1. Gastric lesion
Let’s start with the stomach. The scan reveals an abnormality in the proximal stomach, specifically the gastric fundus. Here, there’s noticeable thickening of the stomach wall, and what’s more concerning is that it extends beyond the wall into the spleen.
This aggressive behaviour strongly points toward malignancy. The first thing that comes to mind is primary gastric carcinoma, though it’s worth noting that this type of cancer usually targets the distal stomach.
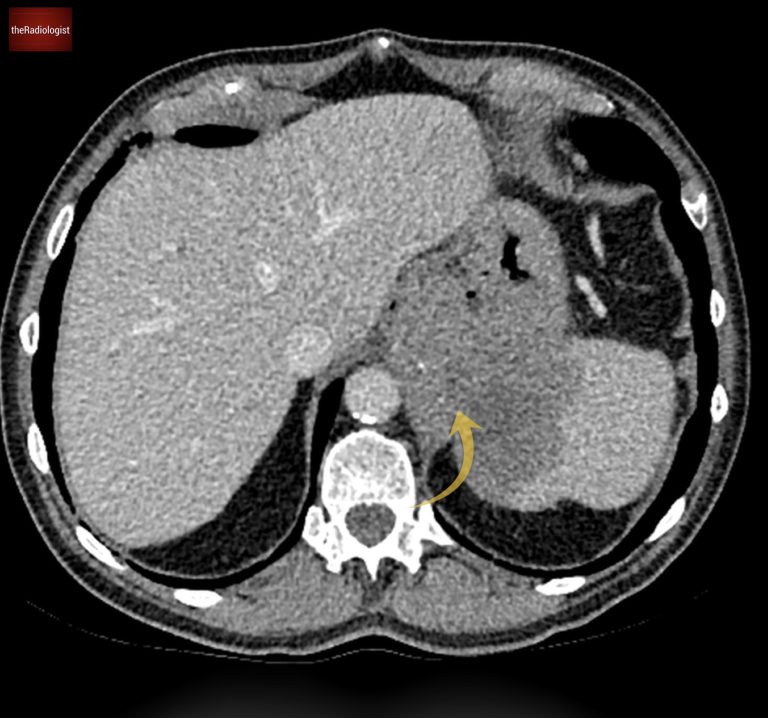
Within the proximal stomach is a lesion that invades the spleen.
2. Small bowel lesion
Moving on to the small bowel, take a closer look at the jejunal loops on the left side of the abdomen. There’s a segment of bowel that looks slightly dilated and shows long-segment thickening of the wall.
Interestingly, the bowel lumen isn’t narrowed, and there’s no significant upstream dilatation, so obstruction doesn’t appear to be an issue here.
Now, when it comes to possible causes, Crohn’s disease and infections can sometimes lead to this kind of thickening. But in light of the abnormality seen in the stomach, we can’t rule out the possibility of a small bowel tumour.
Let’s dive deeper into the different types of small bowel tumours to consider.
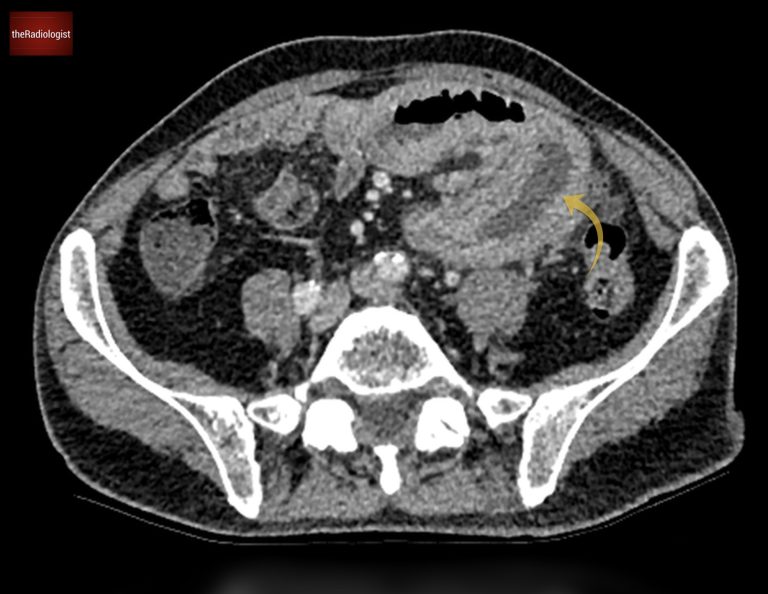
Mural thickening of jejunal loops without narrowing of the bowel lumen.
Small bowel tumours
Let’s have a look at the different types of small bowel tumour:
Carcinoid
- Frequency: The most common small bowel tumour.
- Typical location: Distal ileum.
- Imaging features:
- Small primary lesion with larger mesenteric mass.
- Desmoplastic reaction distorting adjacent bowel loops.
- Potential lymph node enlargement and liver metastases.
Small Bowel adenocarcinoma
- Imaging features:
- Circumferential mural thickening with “shouldering” edges, resembling colonic adenocarcinoma.
- Often associated with obstruction.
- Genetic associations: HNPCC and familial adenomatous polyposis.
Gastrointestinal stromal tumour (GIST)
- Location: More common in the stomach but can involve the small bowel.
- Imaging features:
- Large exophytic masses.
- Typically non-obstructive.
Small bowel lymphoma
- Imaging features:
- Mural thickening with aneurysmal dilatation.
- Bowel obstruction is uncommon as the lumen calibre remains preserved.
- Often associated with enlarged lymph nodes and splenomegaly.
Diagnosis
The presence of both gastric and small bowel lesions raises the suspicion of lymphoma. The jejunal mural thickening without reduction in bowel lumen calibre and lack of obstruction lends weight to the diagnosis.
A PET-CT scan was performed to further evaluate the extent of disease. Let’s go through the findings:
- Gastric mass: Intense FDG avidity confirms active disease.
- Retroperitoneal node: Left para-aortic lymph node shows avid uptake.
- Small bowel: FDG uptake throughout the segment of mural thickening.
These findings reinforce the diagnosis of lymphoma. An upper gastrointestinal endoscopy (OGD) with a biopsy confirmed the diagnosis of lymphoma.
PET-CT shows FDG avidity within the gastric lesion, small bowel loops as well as a left para-aortic lymph node.
KEY POINT
Lymphoma affecting the GI tract often presents with mural thickening without significant lumen obstruction.
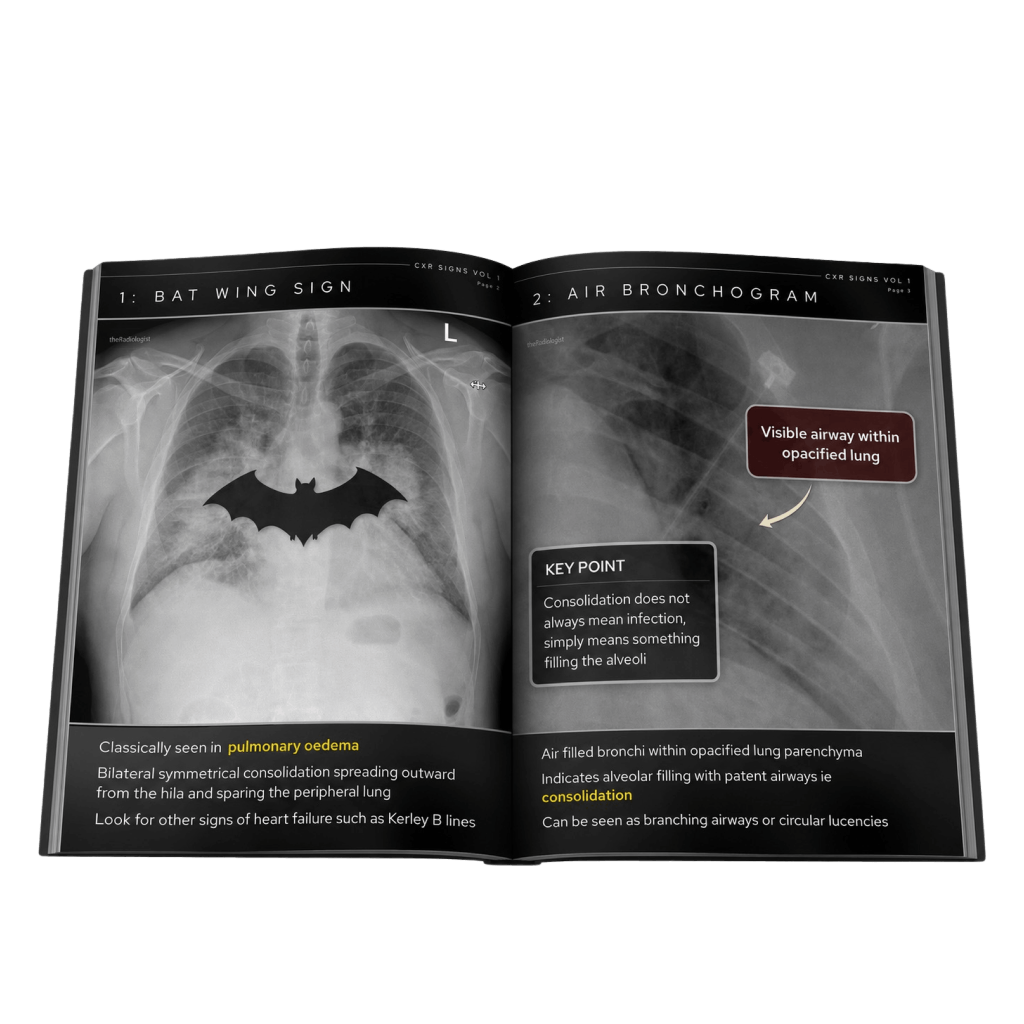
Free guide: 20 Chest X-Ray signs you need to recognise
Downloaded by 10,000+ healthcare professionals.
Get 20 annotated chest X-ray signs with clear teaching points and explanations. Written by a Consultant Radiologist, this free guide is designed to help you recognise important findings more confidently when reviewing chest X-Rays.