A woman in her 50s is brought to the emergency department after a fall and brief loss of consciousness. A non-contrast CT head is performed, followed by a CT angiogram, and there’s something important you don’t want to miss.
In this case, we go through how to spot a subarachnoid haemorrhage from the foramen magnum to the sulci. By the end of this case, you’ll know how to confidently spot subarachnoid haemorrhage on CT and identify key review areas.
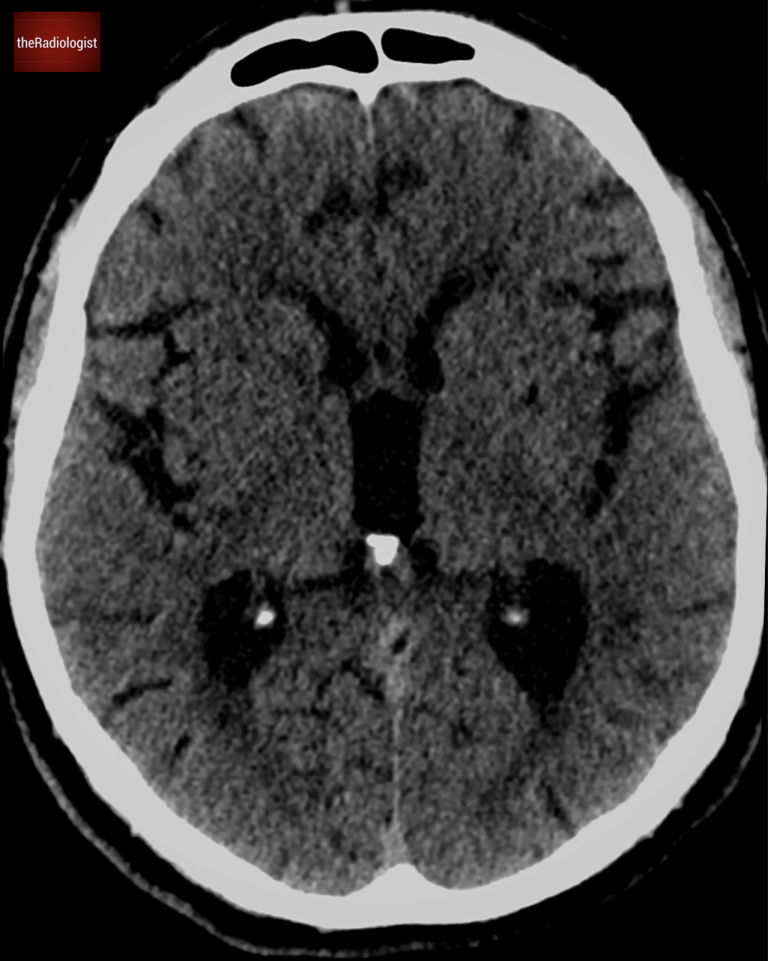
A female in her 50s presents to the Emergency Department after a fall and loss of consicousness. She has a non contrast CT of her brain.
Have a look at the scan below.
I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Now have a look at the post contrast CT angiogram.
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Start by looking at the foramen magnum
I often start at looking at brain CT by looking at the lowest slice. Check to see if you can see the cerebellar tonsils at the foramen magnum – if you do, take a look at the sagittal view and see if there is cerebellar tonsil descent. This could represent an Arnold Chiari malformation or in the acute setting cerebellar tonsil herniation in the context of mass effect. There are no signs of cerebellar tonsil descent in this case.
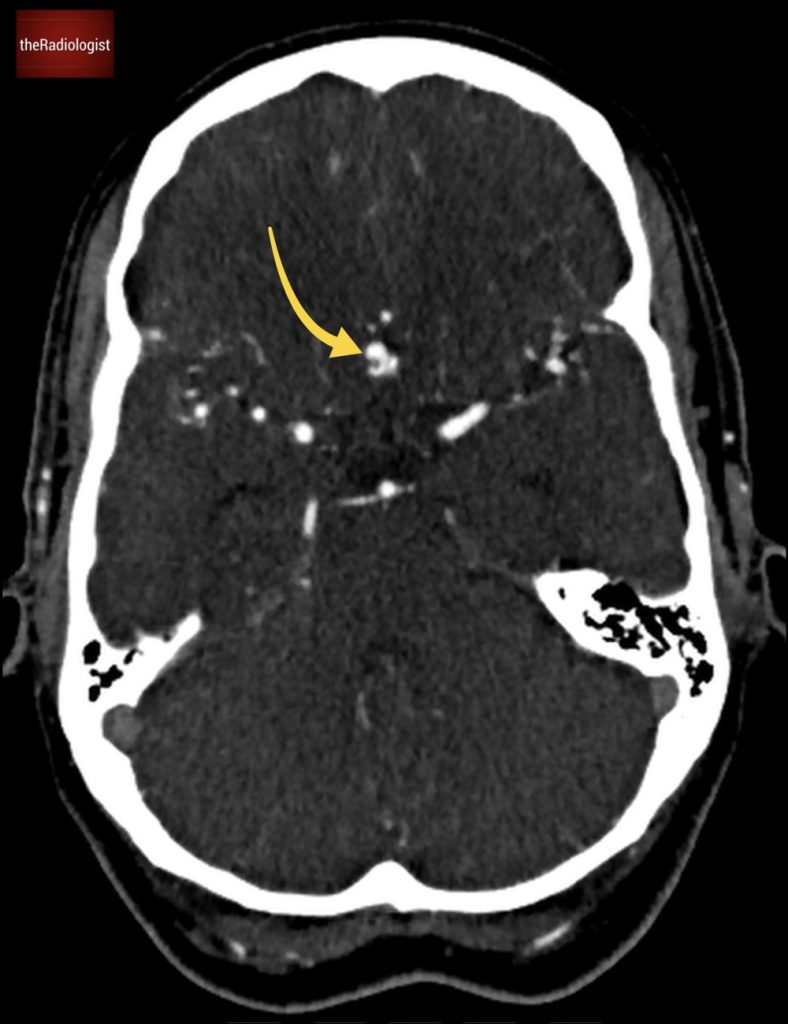
Secondly however, assess for high density CSF in this region. If you do you could be dealing with a subarachnoid haemorrhage and that’s what we have here.
At the foramen magnum, look around the medulla/cervical cord for high density material that can indicate subarachnoid haemorrhage. This case is positive (yellow arrow).
Meningeal anatomy
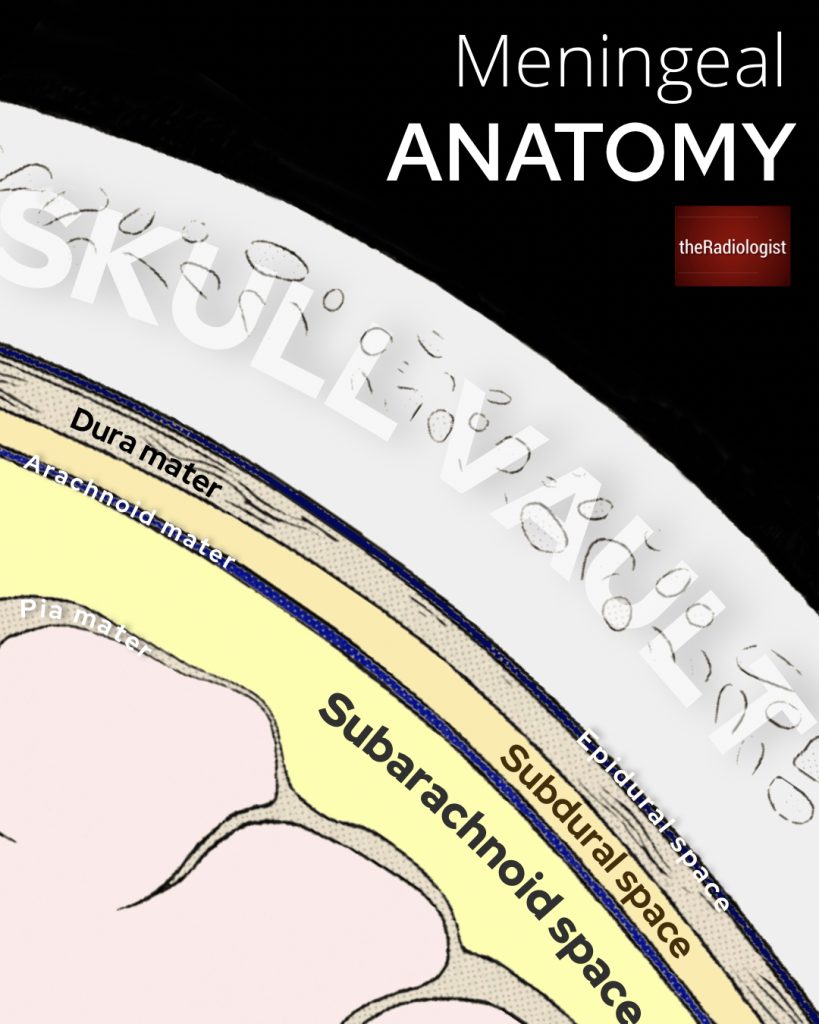
With subarachnoid haemorrhage you have bleeding within the subarachnoid space which lies below the middle layer of the meninges, the arachnoid, and above the pia which is a thin structure that overlies the brain.
Have a look at the diagram below and note the relation of the subarachnoid space to the arachnoid above and pia below.
The subarachnoid space lies over the pia and below the arachnoid.
Review areas
There are many different causes of subarachnoid haemorrhage but the most common by far is a ruptured berry aneurysm.
So how do we look for subarachnoid haemorrhage on a non contrast CT head?
1. Suprasellar cistern
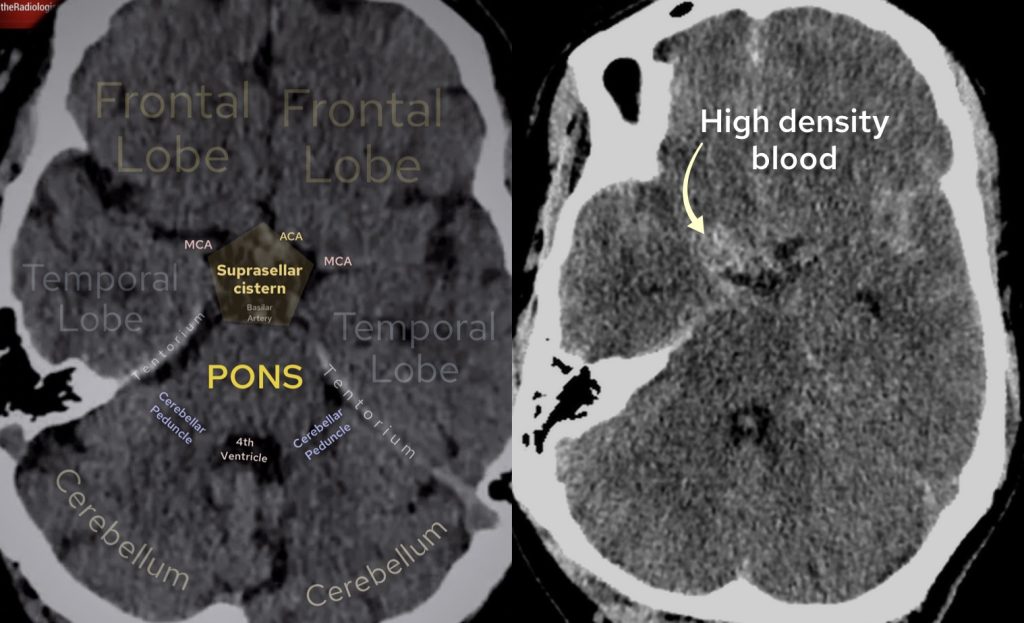
One key review area is the suprasellar cistern. We should see this as a pentagon shaped CSF filled structure but in our case we can’t see it clearly as it is filled with blood. This is subarachnoid haemorrhage.
Have a look at the annotated image of a normal suprasellar cistern on the left – this is normally pentagon shaped and black representing CSF. On the right we have our case where this cistern is filled with high density blood representing acute subarachnoid haemorrhage.
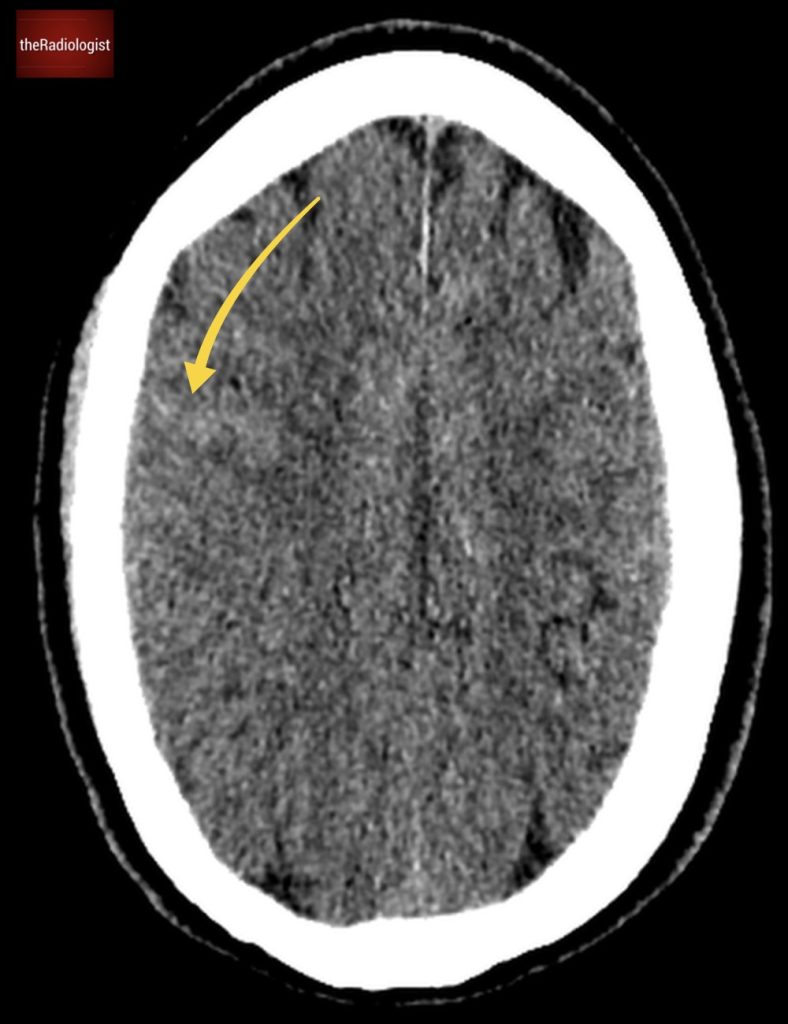
2. Sulci
Subarachnoid haemorrhage can also extend into the sulci like we can see here. This can be quite subtle. To look for this I like to put the scan on a ‘blood window’ (window width 130, window level 45), analyse the thin slices and scroll through slowly looking for asymmetry. Making the scan small can emphasise the asymmetry. Having a look at thick slices as well can help.
Blood within the sulci representing subarachnoid haemorrhage can be tricky to identify on non contrast CT. I find it best to look for this by making the image small comparing side to side and windowing to change to a ‘blood window’ setting.
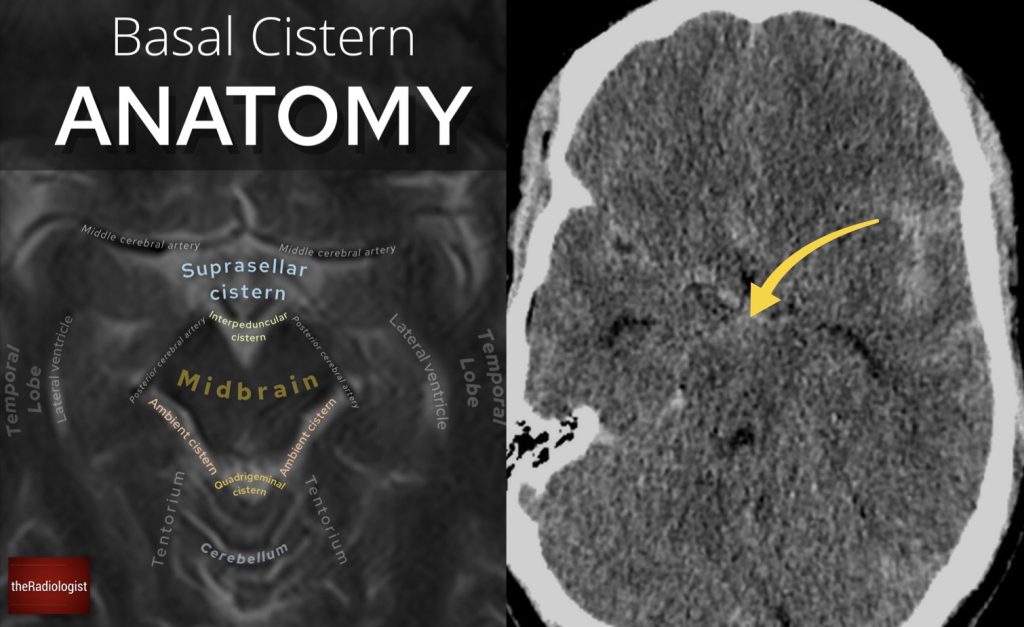
3. Midbrain: between the ‘Mickey Mouse ears’
There is a subset of subarachnoid haemorrhage termed perimesencephalic haemorrhage. This is a venous bleed and there won’t be an abnormality on angiography. The epicentre of the bleed is seen anterior to the midbrain: so I always check in between the ‘Mickey Mouse ears’ of the midbrain for blood. This can be the only finding on the scan and can be very subtle and can be missed.
On the left we have normal anatomy of the midbrain at the level of the interpeduncular cistern on a T2 weighted MRI scan. Look at the normal shape of the ‘Mickey Mouse ears’ of the midbrain. On the right we have our case where we can see high density blood in this region.
Pitfalls
Even when you’re careful, small bleeds can be easy to miss or misinterpret. Here are some common traps to avoid:
1. Artefact at the skull base
The bones around the base of the skull can cause beam hardening artefact that can mimic blood. This is especially common in the posterior fossa and around the temporal lobes. Reconstructing on coronal and sagittal views can help differentiate.
2. Normal veins pretending to be blood
Cortical veins live in the sulci and can look a bit dense on CT, especially in older or dehydrated patients. They usually follow a smooth, straight path. Blood tends to not conform to a linear shape – again reconstructing on sagittal and coronal views can help.
3. Not using the right window settings
The default brain window isn’t always enough. Try a ‘blood window’ (window level 45 and width 130) to make small areas of blood stand out more clearly.
CT head review
In our case you can see there is blood here anterior to the midbrain as well as within the sulci, the basal cisterns.
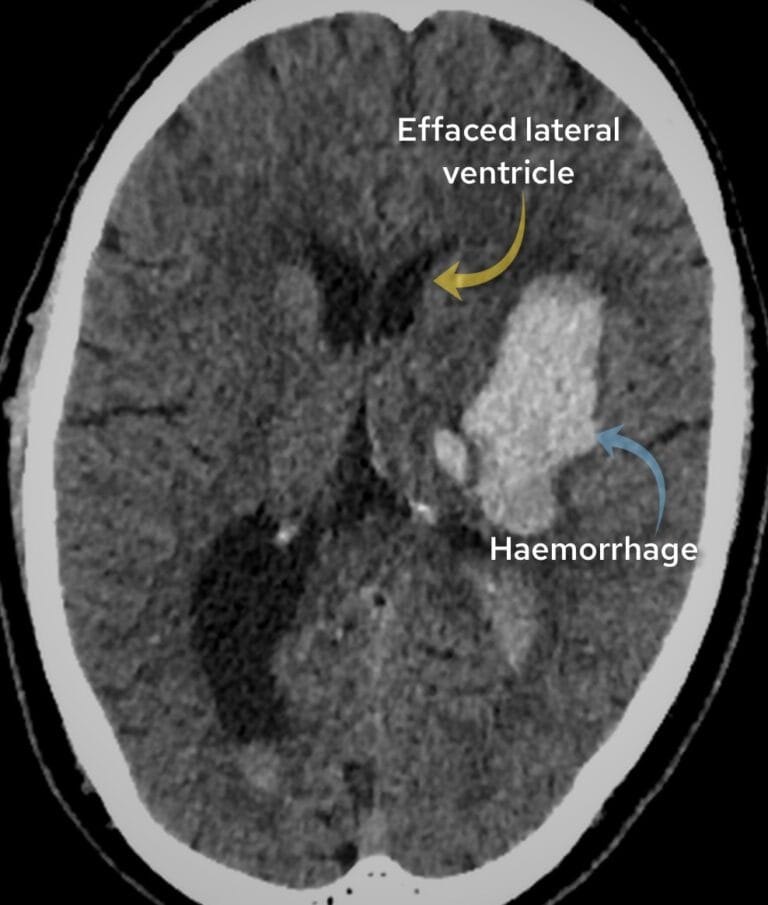
There is even blood extending into the lateral ventricles (see below) and 4th ventricle.
We can see high density blood within the left lateral ventricle.
CT angiogram review
A CT angiogram can be performed to look for an underlying aneurysm. These saccular or berry aneurysms tend to occur at sites of branching and happen at predictable places so it is worth scrutinising a few review areas:
Basilar tip
MCA bifurcation
Junction of anterior communicating artery (ACOM) and anterior cerebral artery (ACA)
In our case we will find a small aneurysm at the junction of ACOM and the ACA (see below).
This was successfully coiled and the patient made a good recovery.
On the post IV contrast images we can see a small aneurysm at the junction of the anterior cerebral artery and anterior communicating artery.
KEY POINTS
Don’t miss a subtle subarachnoid haemorrhage!
My tips would be to change the window to a ‘blood window’ (window level 45 and width 130), make the image small and look for asymmetry as well as interrogating the sulci and basal cisterns.
FREE GUIDE
Free guide: 20 Chest X-Ray signs you need to recognise
Downloaded by 10,000+ healthcare professionals. Get 20 annotated chest X-ray signs with clear teaching points and explanations. Written by a Consultant Radiologist, this free guide is designed to help you recognise important findings more confidently when reviewing chest X-Rays.
You’ve got the framework now let’s put it to work. Dive into a related case to see these findings on real images, or explore another guide to build out your systematic approach. That’s where it really starts to stick.