
Acute appendicitis
How to find and assess an inflamed appendix
Introduction
This CT KUB was done for suspected renal colic, but the key finding wasn’t in the urinary tract. In this case, we show how to assess the right iliac fossa for the appendix, recognise signs of appendicitis, and look for complications like perforation or abscess.
You’ll also learn how to assess for incidental findings on CT KUB, a crucial skill when the primary diagnosis isn’t what you expected.
Case introduction
A male in his 30s presents with right sided abdominal pain. Here is a non contrast CT KUB.
Have a look at the scan below.
I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Assessing for renal tract calculi
Here we have a non contrast CT KUB looking for renal tract calculi. However in this case the kidneys both look normal with no hydronephrosis and no bright renal calculi. If we follow the ureters down there are no definite ureteric calculi. Although there are some right sided pelvic foci of calcification these do not definitely run in the line of the ureter and are more likely phleboliths rather than ureteric calculi.
Make sure you have a look at the bladder as well for calculi – however there are none in this case. There is however an abnormality within the right iliac fossa – always make sure to look for alternative causes of pain.
Assessing the right iliac fossa
When you suspect a right iliac fossa (RIF) abnormality, first start by identifying the caecum. I do this by tracing the colon all the way from the rectum back to the origin. Once you find this, in normal circumstances you will find two things communicating with it. Firstly the terminal ileum and then the appendix.
You should be able to recognise the terminal ileum as communicating with the rest of the small bowel but also look out for some fat density which you will normally find with a normal ileocaecal valve as we can see below.
Find the terminal ileum by identifying the distal small bowel and finding the ileocaecal valve.
When you suspect a right iliac fossa (RIF) abnormality, first start by identifying the caecum. I do this by tracing the colon all the way from the rectum back to the origin. Once you find this, in normal circumstances you will find two things communicating with it. Firstly the terminal ileum and then the appendix.
You should be able to recognise the terminal ileum as communicating with the rest of the small bowel but also look out for some fat density which you will normally find with a normal ileocaecal valve as we can see below.
Separate to the terminal ileum we can see a second structure communicating with the caecum – this is a dilated appendix.
When we follow the appendix in this case we can see it is enlarged with surrounding fat stranding – this is acute appendicitis. It can sometimes be difficult on CT to make the call. I usually use the diameter of the appendix and the presence of surrounding fat stranding to help me make the call. A high density appendicolith within the appendix also adds weight to the diagnosis.
| Diameter | Periappendiceal fat stranding | Diagnosis |
|---|---|---|
| <7 mm | – | Appendicitis not likely: consider other diagnoses |
| >7 mm | – | Indeterminate: consider appendiceal tumour if no acute pain. Look for high density appendicolith which may add weight to appendicitis. |
| >7 mm | + | Acute appendicitis |
Complications and associated findings
One you find appendicitis look for complications:
- Free gas: put on lung windows and make sure there is no perforation
- Collection
Other things to think about when it comes to appendicitis:
- Mucinous neoplasms of the appendix can be asymptomatic and are usually an incidental finding on CT which is why I try and identify the appendix on every abdominal CT I look at. In later stages these can lead to pseudomyxoma peritoneii which will show on CT as ascites with classic scalloping of the liver.
- Neuroendocrine appendiceal tumours can present with features of acute appendicitis although again can be asymptomatic.
- Dropped appendicolith: look out for a retained appendicolith in patients who re-present with abdominal pain after surgery for appendicitis. You may see this away from the surgical site.
- Stump appendicitis: consider when there are features of appendicitis after an appendectomy. Here there is recurrent appendicitis affecting residual appendiceal tissue.
Incidental findings
Did you spot the other incidental findings? Firstly there are gallstones within the gallbladder.

The yellow arrow shows us a gallstone within the gallbladder.
There is an umbilical hernia but most importantly there is a soft tissue lesion within the subcutaneous tissues which was worked up after the scan, resected and proven to be a soft tissue sarcoma.
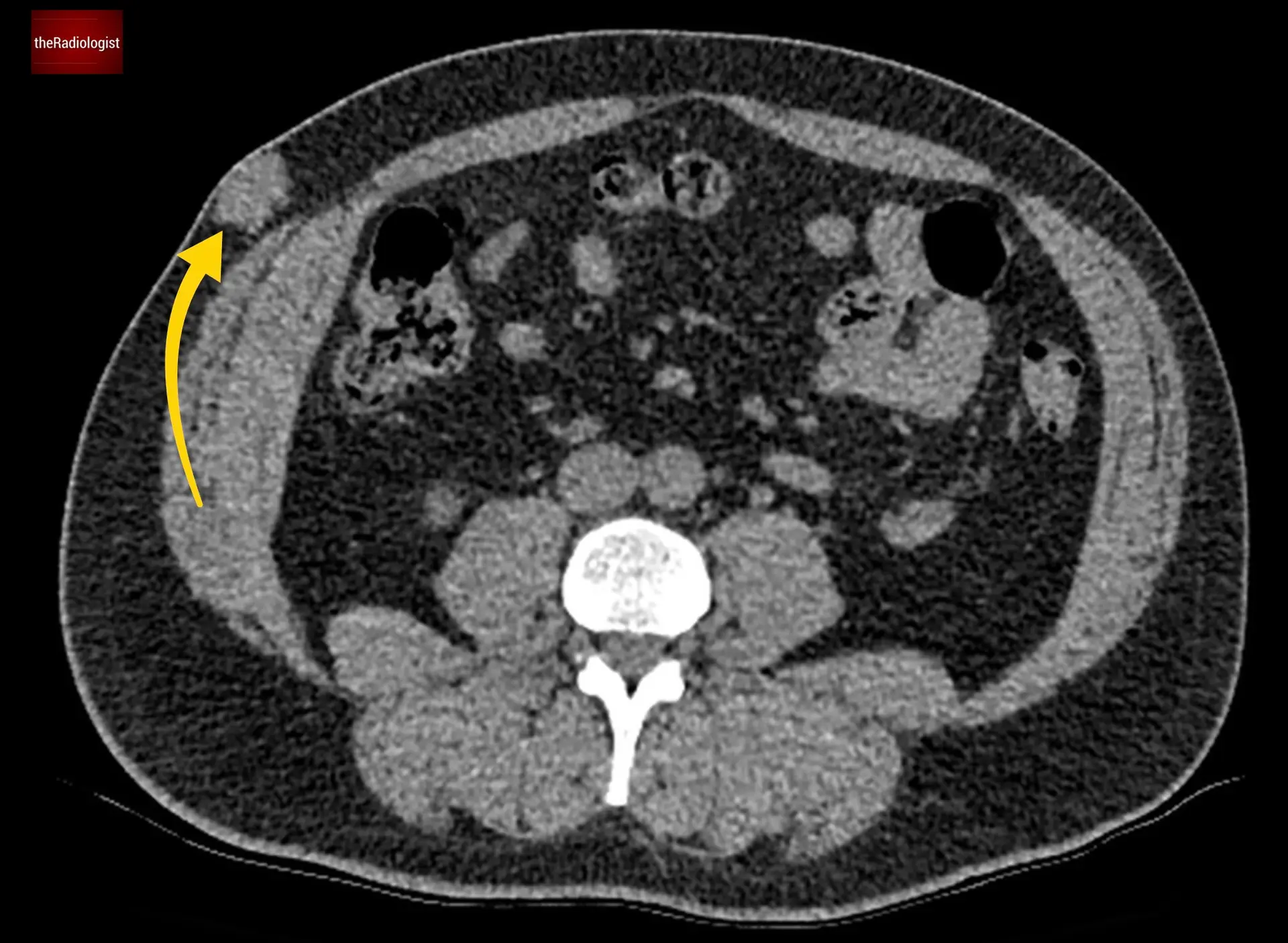
Remember to assess the peripheral soft tissues on CT: here we have an incidental lesion which later proved to be a sarcoma, thankfully resected early.
KEY POINTS
In normal circumstances you should find two structures communicating with the caecum: the terminal ileum which heads to the ileocaecal valve with its characteristic fat density as well as the appendix.