Bone lesions on X-ray can be difficult to interpret. With a wide range of possible causes, it helps to have a clear, structured approach that takes the guesswork out of the process. The key is to know what makes an aggressive versus a non-aggressive lesion.
In this case, we go step by step through the X-ray of a 50-year-old man with ankle pain, using six key features to assess the lesion.
You’ll learn how to recognise aggressive patterns, narrow your differential diagnosis, and identify signs that point toward metastatic disease.
A man in his 50s presents with ankle pain. Have a look at the two views of his X-Ray – are there any worrying findings?
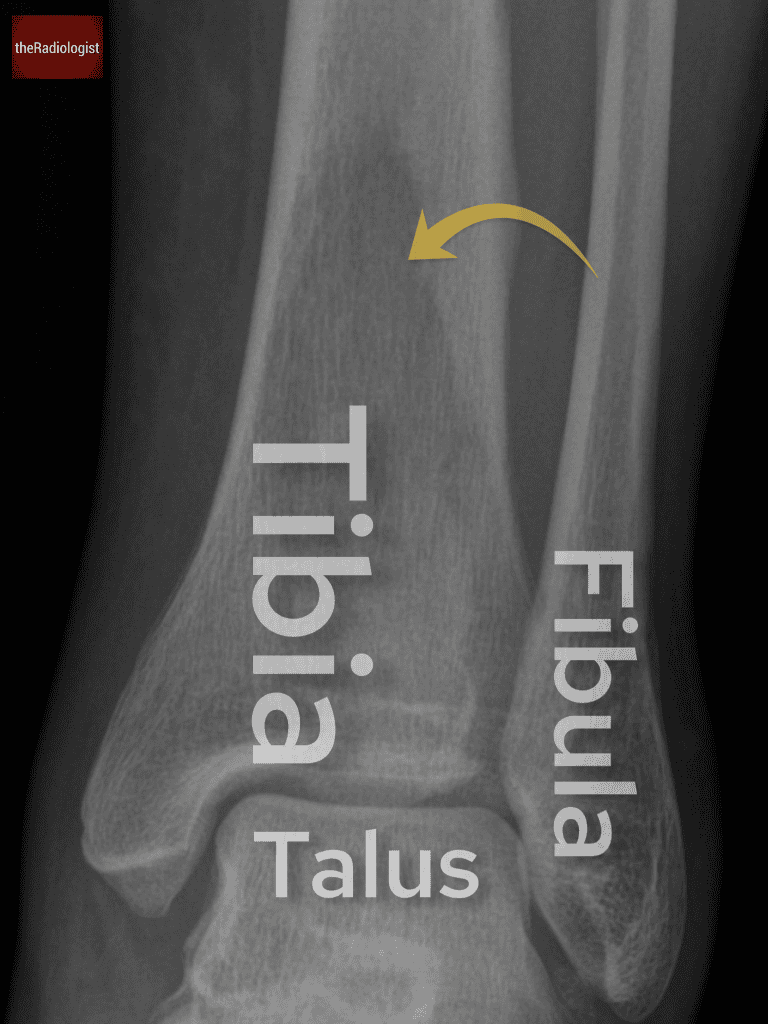
AP view
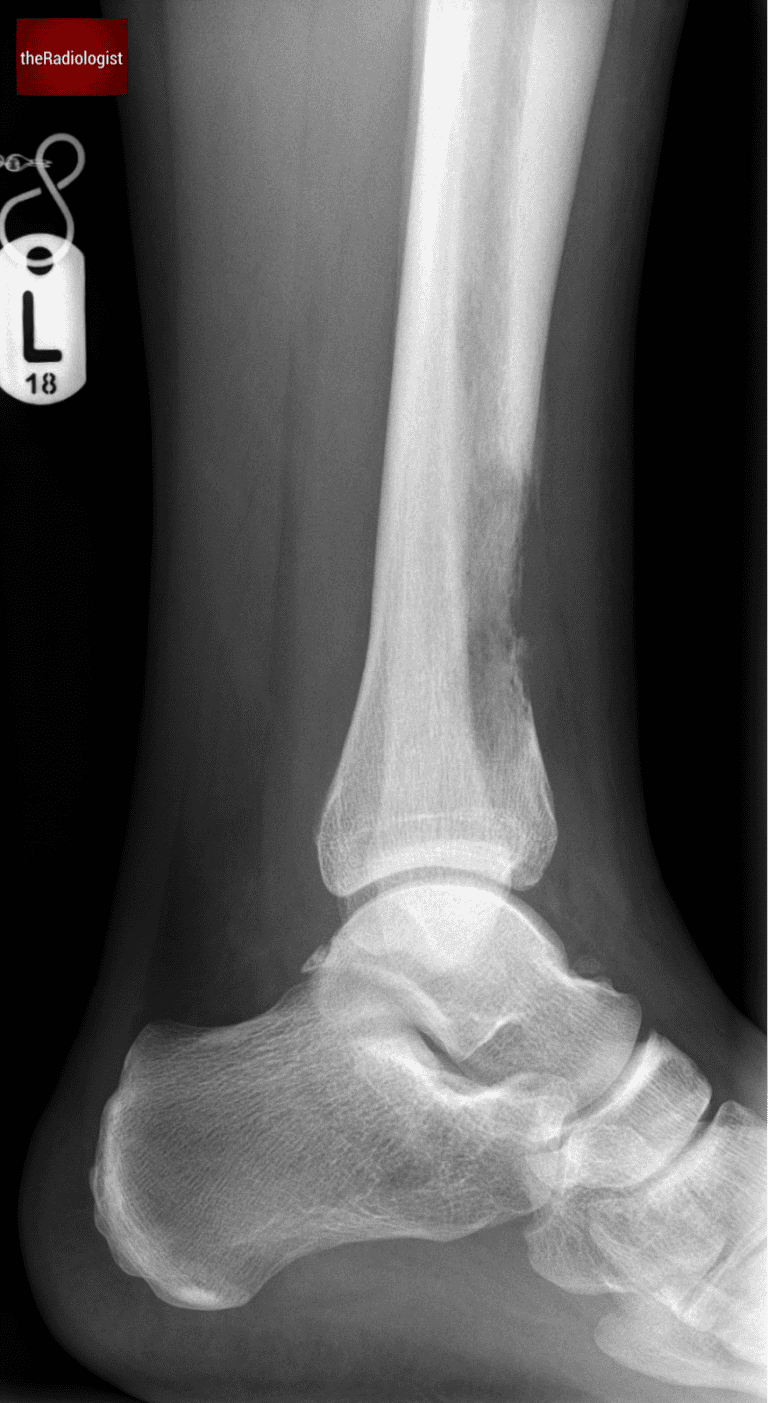
Lateral view
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Initial findings
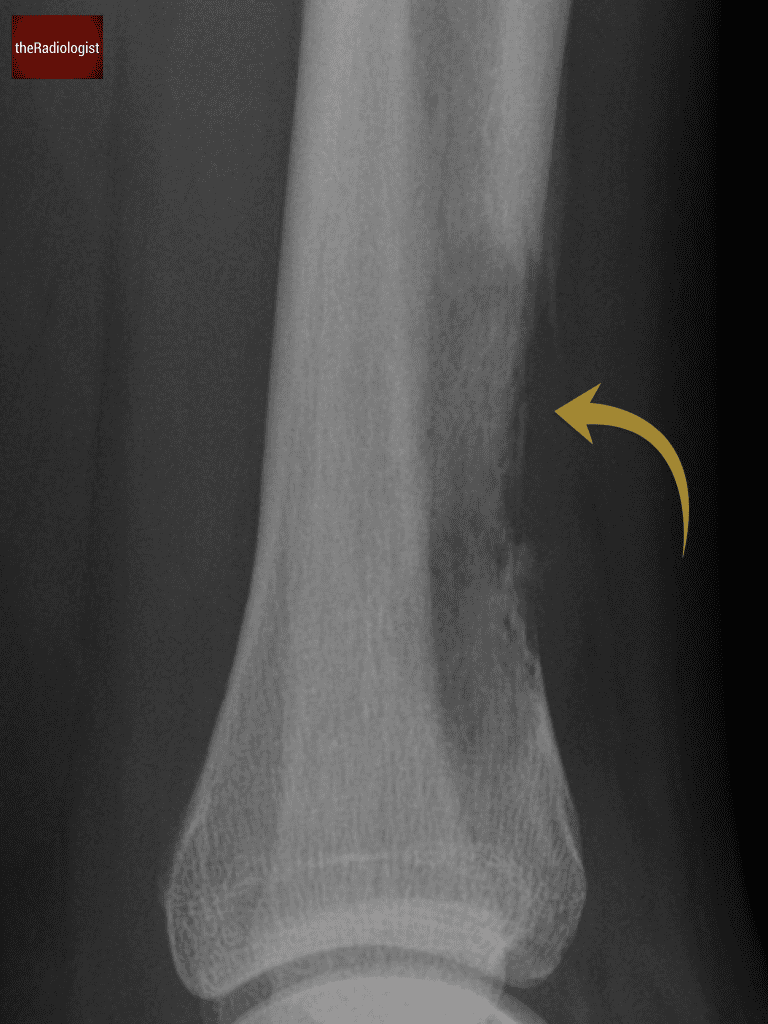
This X-ray shows a lesion in the distal tibia, seen on both the frontal and lateral views.
Seeing a bone lesion can be daunting but let’s go through a system to try and make it more straightforward. The key is to discriminate between an aggressive versus a non-aggressive lesion.
There is a lucent lesion within the distal tibia.
Assess six key features
To systematically evaluate any bone lesion on X-ray, consider these six features:
1. Growth plates
The first step is to determine if the growth plates are fused, as this impacts the differential diagnosis. In this case, the patient is an adult, so we’re dealing with a mature skeleton.
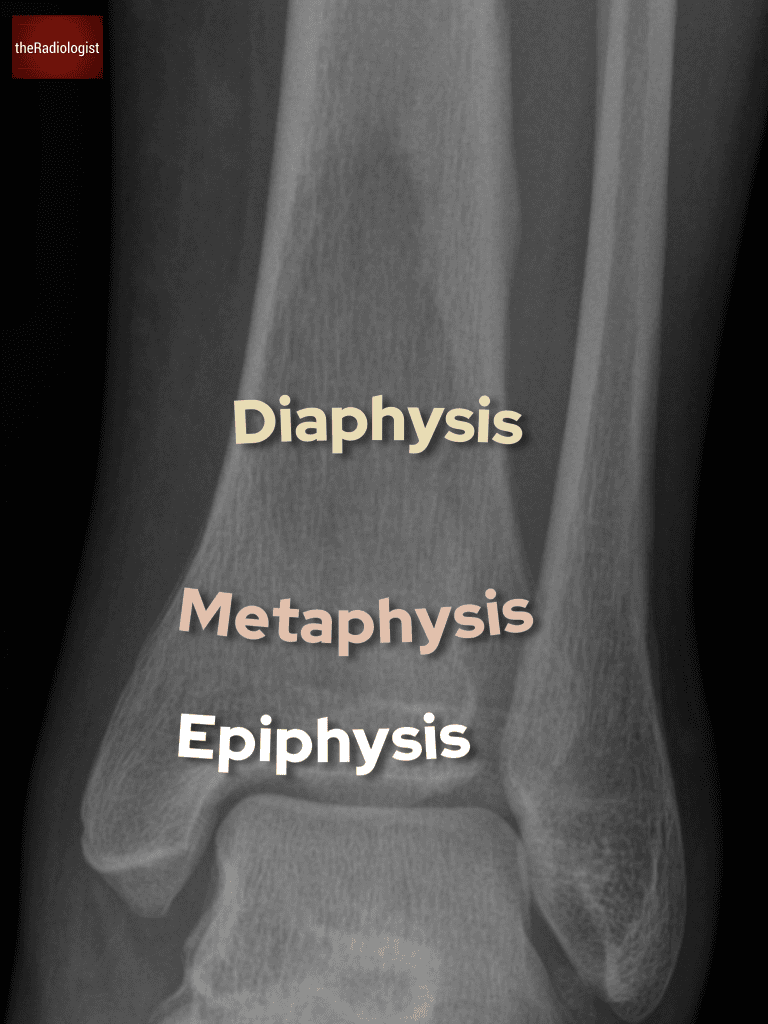
2. Location
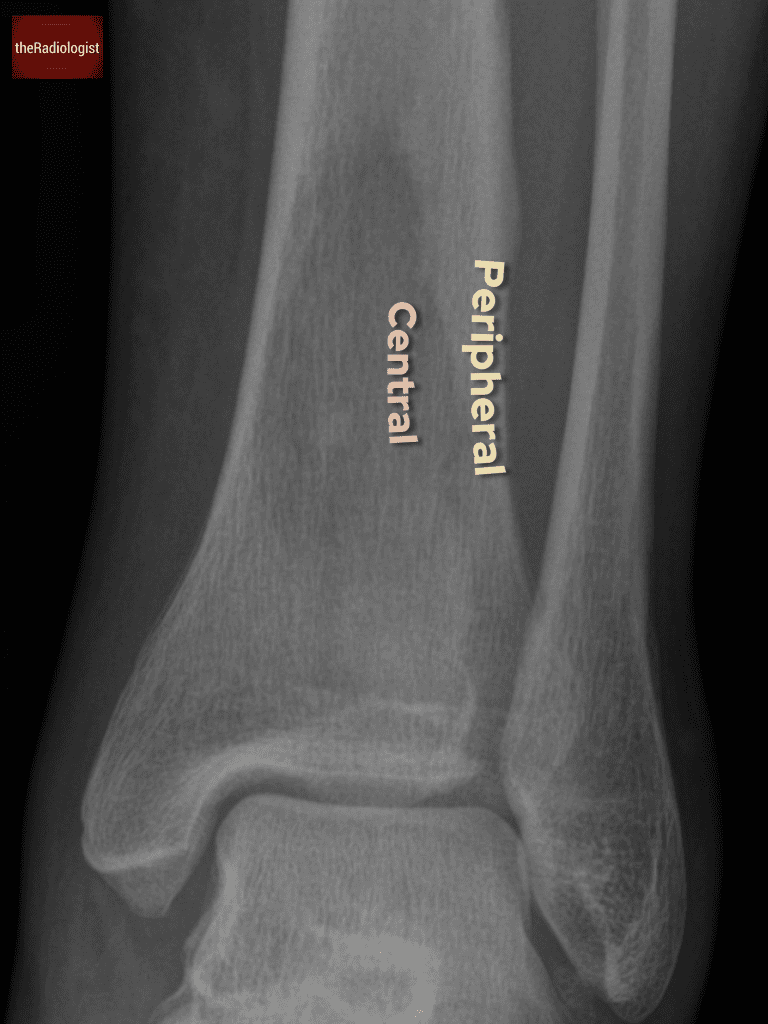
Identify whether the lesion is located in the metaphysis, diaphysis, or epiphysis, and whether it is central or peripheral.
Here, the lesion is predominantly in the diaphysis and is peripheral, closer to the cortex.
Describe whether the lesion lies within the epiphysis, metaphysis or diaphysis.
Also describe whether the lesion is peripheral or central.
3. Bone destruction
Assess the extent and pattern of bone destruction.
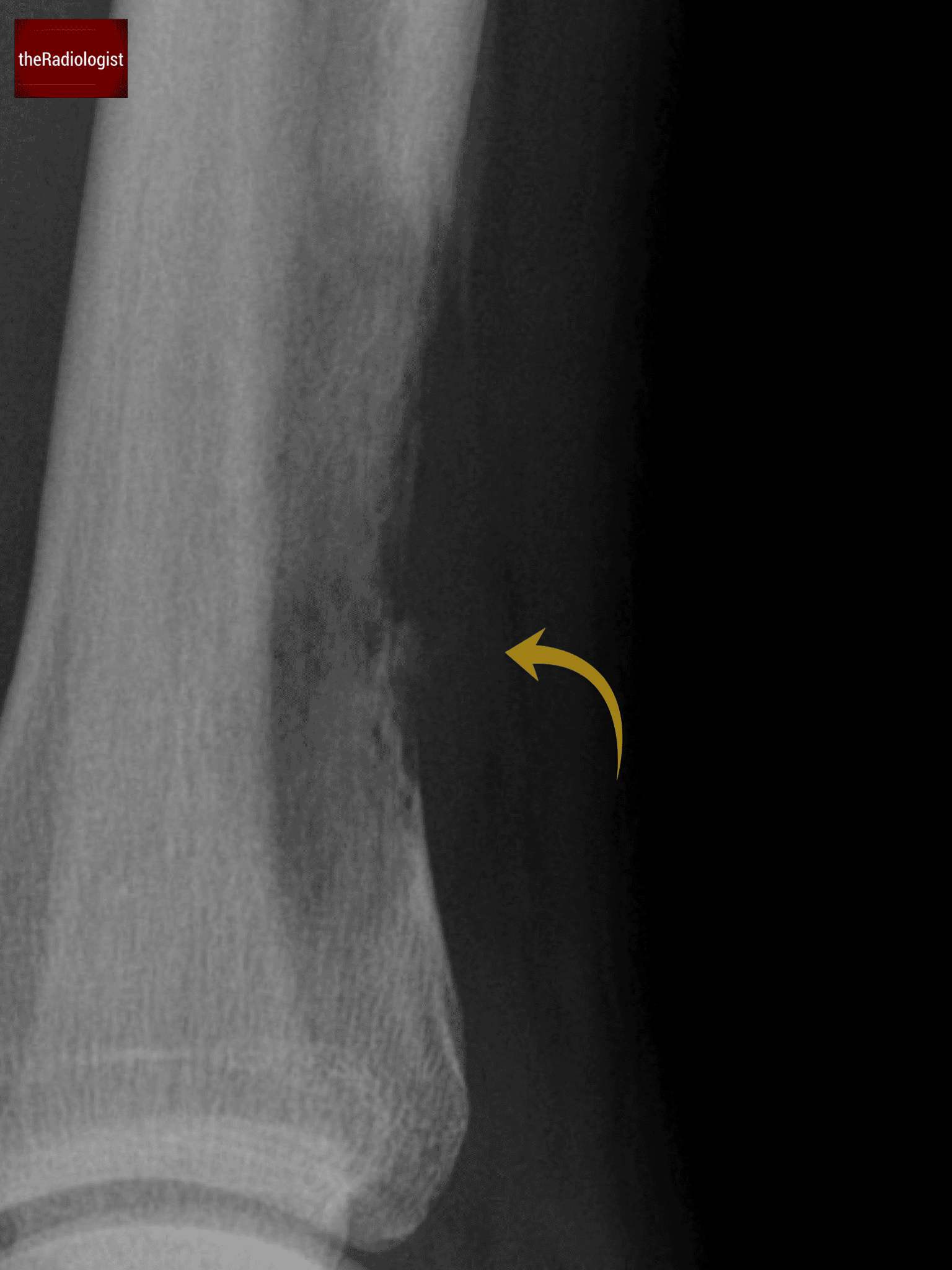
In this case, there is complete destruction of the cortex, a hallmark of an aggressive lesion.
Have a look at the lateral view and you will see some bone missing: bone destruction suggests an aggressive lesion.
4. Zone of transition
Examine the borders of the lesion. A narrow zone of transition means you could outline the lesion with a pencil, suggesting a more benign process.
This lesion, however, has a wide zone of transition at its superior and inferior borders, which is a sign of an aggressive lesion.
Have a look at the lateral view and you will see some bone missing: bone destruction suggests an aggressive lesion.
5. Periosteal reaction
Periosteal reaction on its own is not a good differentiator: thick periosteal reaction is often benign but there are more aggressive patterns.
The lateral view shows a Codman triangle, where a sliver of periosteum is elevated from the cortex. This is an aggressive periosteal reaction, often seen in malignancy or osteomyelitis.
Once you see a Codman triangle, you know you are dealing with an aggressive lesion.
6. Soft tissue mass
Search for evidence of a soft tissue mass, which further supports an aggressive diagnosis.
On the lateral view, there appears to be the outline of a soft tissue lesion adjacent to the area of cortical destruction.
It is tricky but there is possibly a soft tissue lesion associated with the region of bone destruction.
Differential diagnosis
The combination of bone destruction, a wide zone of transition, and a Codman triangle strongly suggests an aggressive lesion. The key differentials include:
1. Bone metastasis
Bone metastases are the most common cause of aggressive bone lesions in adults.
In this case we have a lytic lesion meaning if this is a metastasis we should consider renal cell carcinoma and lung cancer in a male.
2. Multiple myeloma
Another common cause of lytic bone lesions, though it typically presents with multiple lesions.
3. Osteomyelitis
Infection can look similar to a malignant lytic lesion on X-Ray but the clinical situation is usually different.
4. Primary bone tumours
Osteosarcoma: Unlikely here due to the patient’s age. Osteosarcomas more commonly affect adolescents and young adults.
Chondrosarcoma: A possibility, though we might expect ring-and-arc calcifications, which are absent in this case.
Given the aggressive features, the leading differential is a bone metastasis but what cancers are we thinking about?
Cancers that metastasise to bone
X-ray shows a lesion in the distal tibia, seen on both the frontal and lateral views.
Seeing a bone lesion can be daunting but let’s go through a system to try and make it more straightforward. The key is to discriminate between an aggressive versus a non-aggressive lesion.
Lytic or sclerotic
Cancer
Notes
Lytic
Lung
Renal
Classically ‘expansile’
Thyroid
Sclerotic
Prostate
Mixed sclerotic and lytic
Breast
CT scan assessment
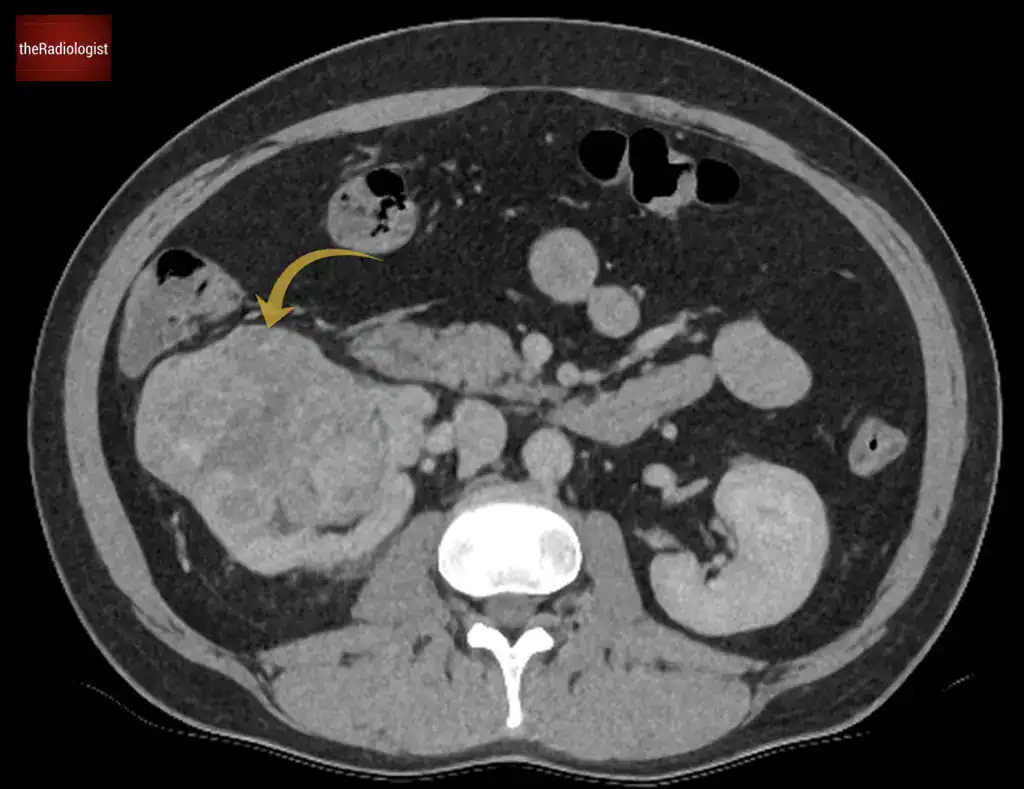
A CT scan was performed to investigate the source of the metastasis. It revealed a large tumor associated with the right kidney, confirming the diagnosis of renal cell carcinoma (RCC)with metastatic bone disease.
Body CT showed an aggressive lesion within the right kidney, proven to represent a renal cell carcinoma (RCC).
KEY POINTS
When you find a suspicious bone lesion on X-Ray, assess it by using the six key features which can help you narrow down the differential diagnosis.
If you see a suspicious sclerotic lesion the differential changes according to the sex of the patient. If a male think prostate cancer. In a female consider breast cancer.