Early MCA territory infarcts
On CT head
Introduction
A man in his 60s presents with sudden right-sided weakness. A non-contrast CT head is performed to rule out haemorrhage or mass, but there’s more to see if you know where to look.
In this case, we break down how to identify key early CT features of an MCA infarct, including the insular ribbon sign and hyperdense MCA sign, and how to use CT angiography to confirm vessel occlusion. A must-know review for recognising stroke early and improving patient outcomes.
Case introduction
A man in his 60s presents to the emergency department with sudden right-sided weakness. A non-contrast CT of the head is performed—what does it show?
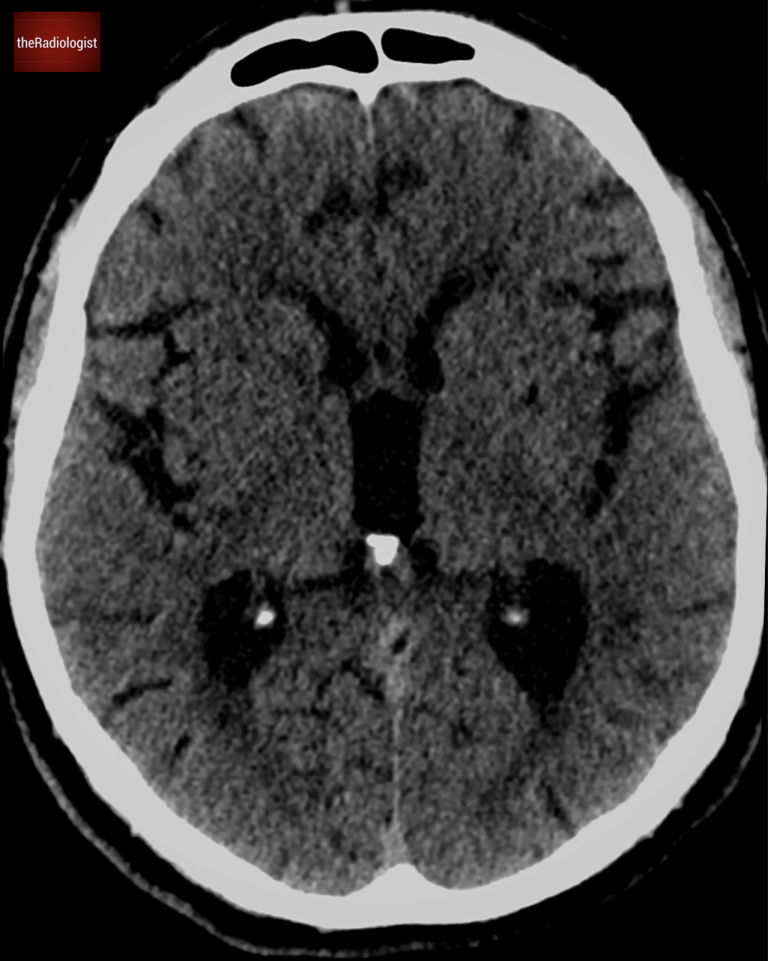
Axial slice of a non contrast brain CT at the level of the 3rd ventricle. Does it show an abnormality?
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Assessing for ischaemic stroke on CT
When a patient presents with sudden weakness, stroke is high on the list of possible causes. A non-contrast CT head is typically the first imaging modality used in these cases. While an early ischaemic stroke may not always be visible on CT, the key role of this scan is to rule out haemorrhage or a space-occupying lesion as the cause of symptoms (remember that IV contrast may mask high density blood so we want a non contrast scan in the first instance).
There are some subtle CT signs that can help identify an early stroke within the first few hours.
Circle of Willis anatomy
Approximately 85% of strokes are ischaemic, caused by a thrombotic or embolic occlusion of a cerebral artery. Given its large territory, the middle cerebral artery (MCA) is the most commonly affected vessel in embolic strokes.
While some patients present with the classic stroke symptoms—hemiparesis, facial droop, or speech difficulties—others may have more subtle presentations. Recognizing the early signs of an MCA stroke is essential for timely intervention – I have seen subtle early stroke signs missed on scans where it has not been expected which then has implications on patient management.
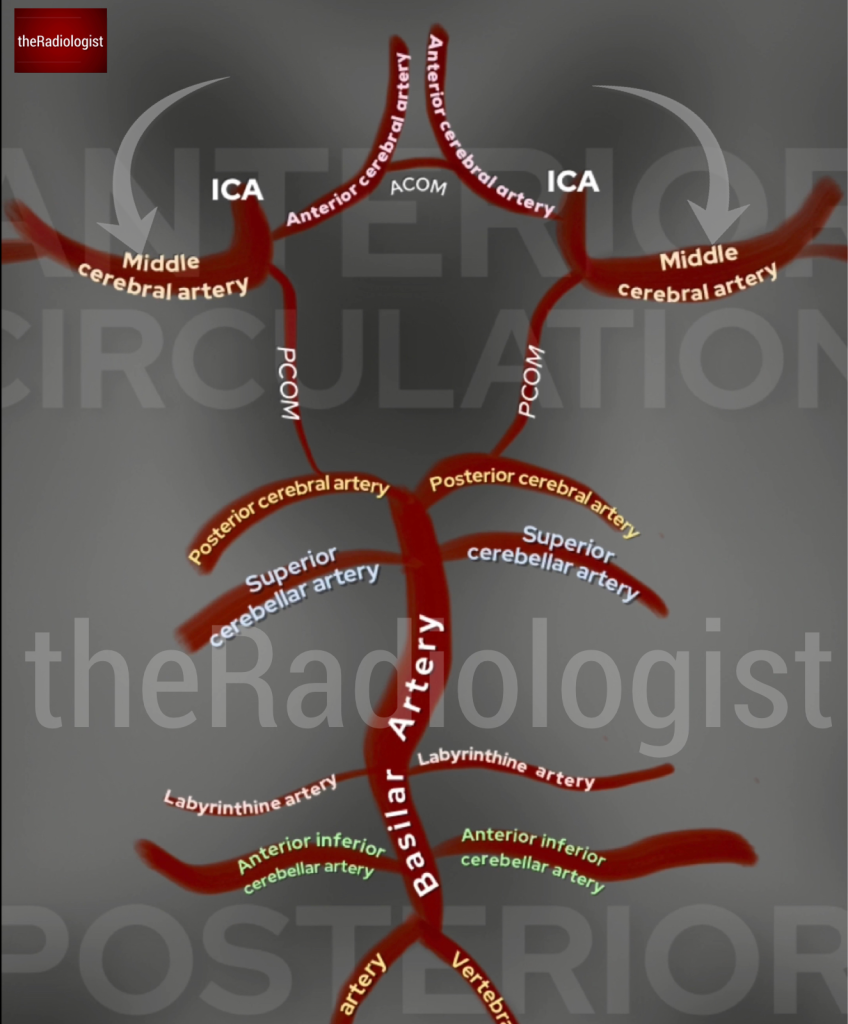
Annotated image of part of the Circle of Willis showing the middle cerebral arteries. The internal carotid artery coming up from the neck divides into the middle and anterior cerebral arteries.
Early signs of an MCA territory infarct
In general early signs of an acute stroke include loss of grey-white matter differentiation and effacement of the sulci. However let’s look at two more specific signs of an MCA stroke on CT that are seen in the very early stages:
- The hyperdense MCA sign
- The insula ribbon sign
1. The Hyperdense MCA Sign
One of the earliest indicators of an MCA stroke is a hyperdense MCA sign: a visible thrombus within the vessel, seen in the image below as a bright segment in the Sylvian fissure.
If you suspect a hyperdense MCA, compare it with the same artery on the opposite side. A clear density difference suggests an acute thrombus.
Remember this applies on non-contrast scans not post-contrast where you would expect the opposite and a filling defect or loss of the vessel altogether.
Going back to our case on the right sided image below, looking at both middle cerebral arteries, they appear equal in density, so there is no hyperdense MCA sign present.
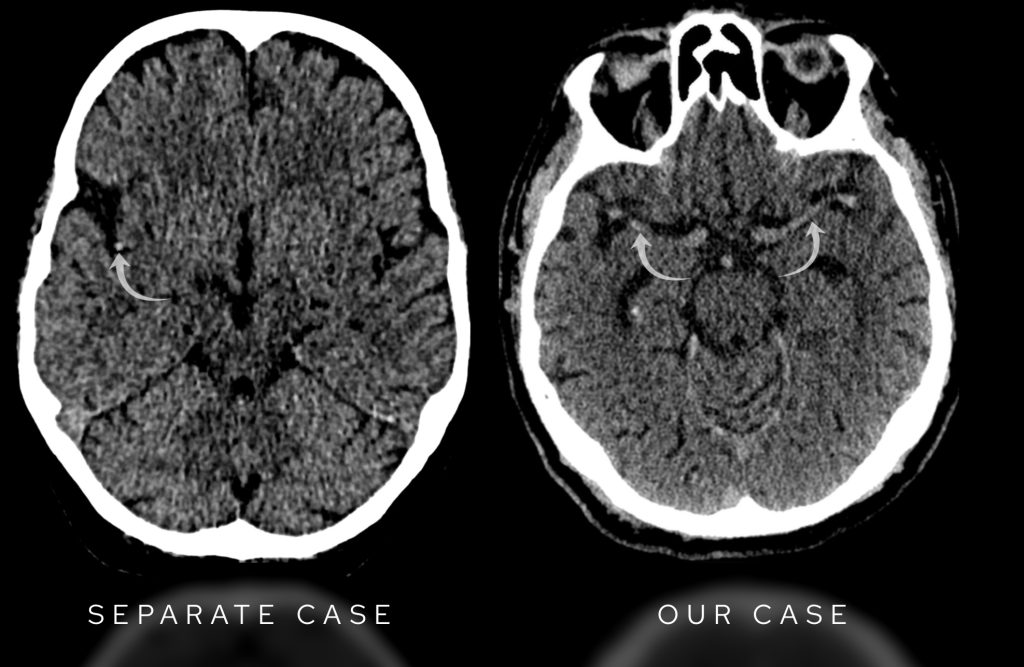
On the left we have an example of a positive right sided hyperdense MCA in a case of acute stroke. In our case on the right sided image, the middle cerebral arteries are equal in density and considered normal.
2. The Insula Ribbon Sign
The insula cortex is an important area to examine in MCA strokes. It is supplied by small perforating branches from the M2 segment of the MCA and is particularly vulnerable to ischaemia because it has limited collateral circulation.
What do we look for?
Normally, the insula cortex is slightly brighter than the internal capsule on a non-contrast CT. If this distinction is lost, it is an early indicator of an MCA infarct—this is called the “loss of the insula ribbon” sign.
In our case the right insula looks normal—slightly brighter than the internal capsule. But on the left, the insular cortex is indistinguishable from the internal capsule—suggesting early infarction.
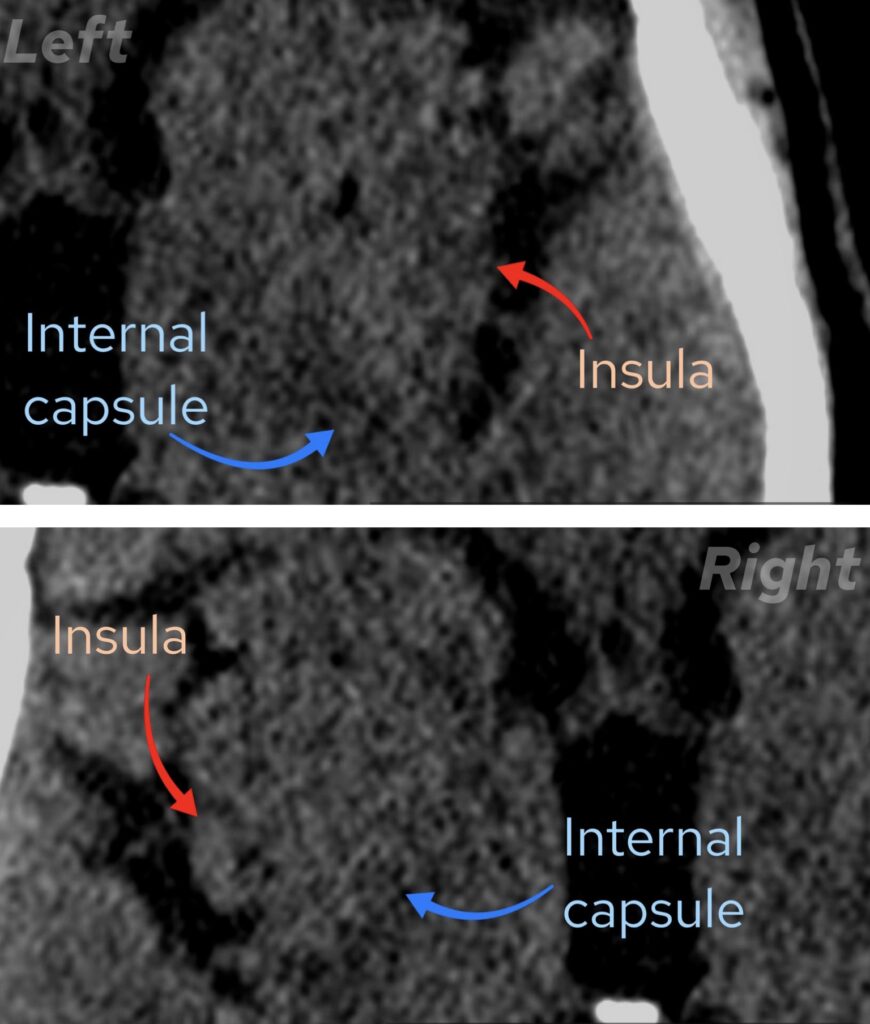
On the left (top image) the insula is a similar density to the internal capsule but on the right (bottom image) we can see it is brighter ie how it should be: there is ‘loss of the insula ribbon’ on the left, an early sign of MCA infarction
CT angiogram findings
To assess the blood vessels, a CT angiogram (CTA) was performed.
What do we look for on a CT angiogram performed in the context of possible MCA stroke?
The internal carotid artery (ICA) should be patent before it divides into the anterior cerebral artery (ACA) and middle cerebral artery (MCA). Follow the M1 segment of the MCA as it moves laterally toward the Sylvian fissure. Look for a sudden cutoff in the artery, suggesting an occlusion.
In our case the right MCA appears normal. On the left, we can see the M1 segment, but the artery disappears as it transitions into the M2 segment: this confirms an acute MCA occlusion. Have a look at the scan below:
Follow the left sided ICA into the M1 segment of the MCA and you will find it becomes occluded
Early diagnosis is key
Sometimes a stroke diagnosis is obvious based on the clinical picture, but in other cases, the symptoms can be more subtle. Spotting early CT signs, such as loss of the insula ribbon or a hyperdense MCA, can be crucial in initiating timely treatment such as thrombectomy or thrombolysis, potentially making the difference between full recovery and severe disability.
Usually thrombolysis should be delivered within 4.5 hours of symptom onset and thrombectomy is best done within 6 hours but can be performed within 24 hours in select cases.
In general faster treatment leads to better outcomes so keep on looking for those insula ribbons!
Middle cerebral artery anatomy
Before we close let’s take a minute to think about the middle cerebral artery: see the image below.
Why is it important to know about the anatomy of the MCA?
As the internal carotid artery reaches the Circle of Willis it divides into the anterior cerebral artery and the middle cerebral artery – as the larger and more direct branch, the MCA is prone to embolism and is commonly involved in ischaemic stroke.
After arising from the internal carotid artery, the first segment of the MCA is the horizontal segment (M1) which gives off multiple lenticulostriate arteries which supply the basal ganglia. Notice how some of the medial lenticulostriate vessels arise from the ACA including the recurrent artery of Heubner. Lenticulostriate embolism is relatively common usually resulting in lacunar infarction, typically affecting just motor function.
The MCA then bifurcates into superior and inferior divisions, although where this occur can vary and may happen along the insular segment (M2). Aneurysms can occur at the bifurcation so always interrogate this region.
The vessel then courses laterally as the M3 (opercular) segment and finally the M4 (cortical) segment.
On non-contrast CT I look at the MCA on every scan checking for a hyperdense segment that could represent an acute thrombus as well as looking for an incidental aneurysm that you may be able to see without IV contrast.
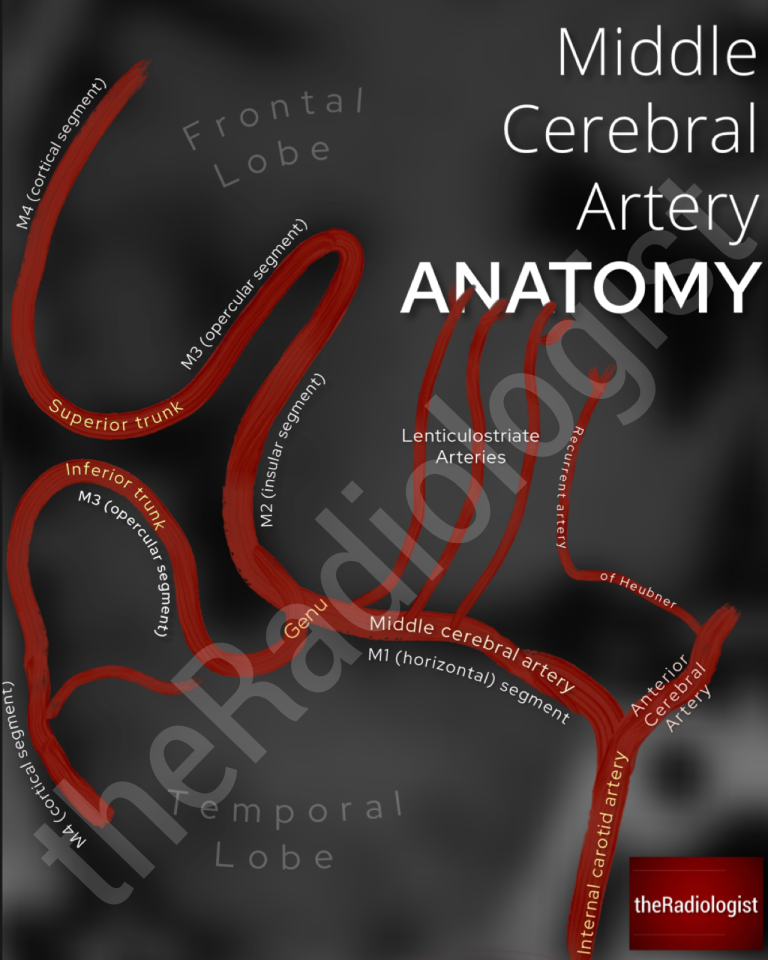
Diagram showing the anatomy of the middle cerebral artery.
KEY POINTS
Don’t miss the insula from your standard review of a CT head.
Of course this should form part of your search pattern in any possible stroke case but I include this on every CT head I look at and have picked up early MCA stroke where it hadn’t been initially suspected.
Using thick 5 mm slices and ‘stroke windows’ can help assess when you are not sure.