
Colloid cysts
On brain CT and MRI
Introduction
A woman in her 50s comes in with a persistent headache and a wobbly gait. Her GP sends her for an urgent brain MRI, and the scan shows something small but serious that needs immediate attention.
This case breaks down how to read the MRI, spot signs of acute hydrocephalus, and think through the key differentials.
Whether you’re in radiology, neurology, or just want to sharpen your MRI skills, this is a case worth knowing.
Case introduction
A woman in her 50s, with no significant medical history, visits her GP complaining of a persistent headache and an altered gait. Given her symptoms, she undergoes an urgent MRI of the brain. Shortly after the scan, she is admitted to the hospital.
Have a look at the axial FLAIR images of the scan below. What does it show?
I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Assessing FLAIR images on MRI
One of the key sequences used in brain imaging is FLAIR (Fluid Attenuated Inversion Recovery). It’s a variation of T2-weighted imaging but with fluid (like CSF) suppressed, making it excellent for detecting inflammation and oedema. Have a look at the images below and compare the fluid within the CSF, the grey matter and the white matter.
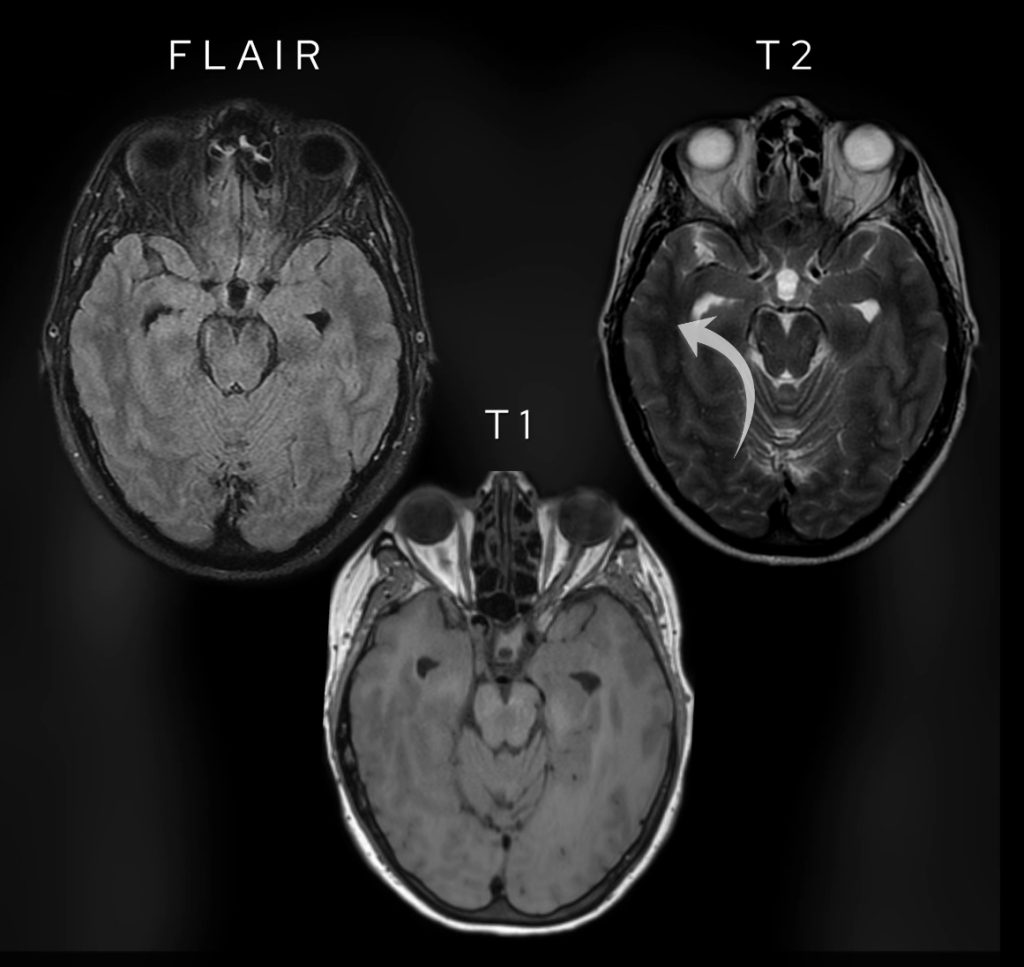
Note the difference between FLAIR images and T1 weighted and T2 weighted images. Fluid is dark like on T1 weighted images. Note the white matter (arrowed on the T2 image) is brighter than grey matter only on T1 weighted images.
Like on T2-weighted images, oedema shows as bright but unlike T2-weighted images fluid is dark (as can be seen on T1-weighted images). Have a look at the table below which highlights some of the key differences.
| Sequence | Fluid | White versus grey matter | Oedema | Fat |
|---|---|---|---|---|
| T1-weighted | Dark | White brighter than grey | Not seen | Bright |
| T2-weighted | Bright | White darker than grey | Bright | Bright |
| FLAIR | Dark | White darker than grey | Bright | Dark |
Hydrocephalus
In this case, we immediately notice marked dilation of the lateral ventricles, an important clue. However, when we look further down at the fourth ventricle, it appears normal in size.
This suggests obstructive hydrocephalus, meaning something is blocking the normal flow of cerebrospinal fluid (CSF). What’s causing the obstruction?

The lateral ventricles are dilated but the 4th ventricle is normal in calibre suggesting there is obstructive hydrocephalus.
Have a look at the normal annotated brain scan below and compare it to our case.
A normal brain scan shows that the foramen of Monro connects the lateral ventricles to the third ventricle. However, in our patient’s scan, there is a well-defined lesion in the roof and anterior aspect of the third ventricle, right at the foramen of Monro.
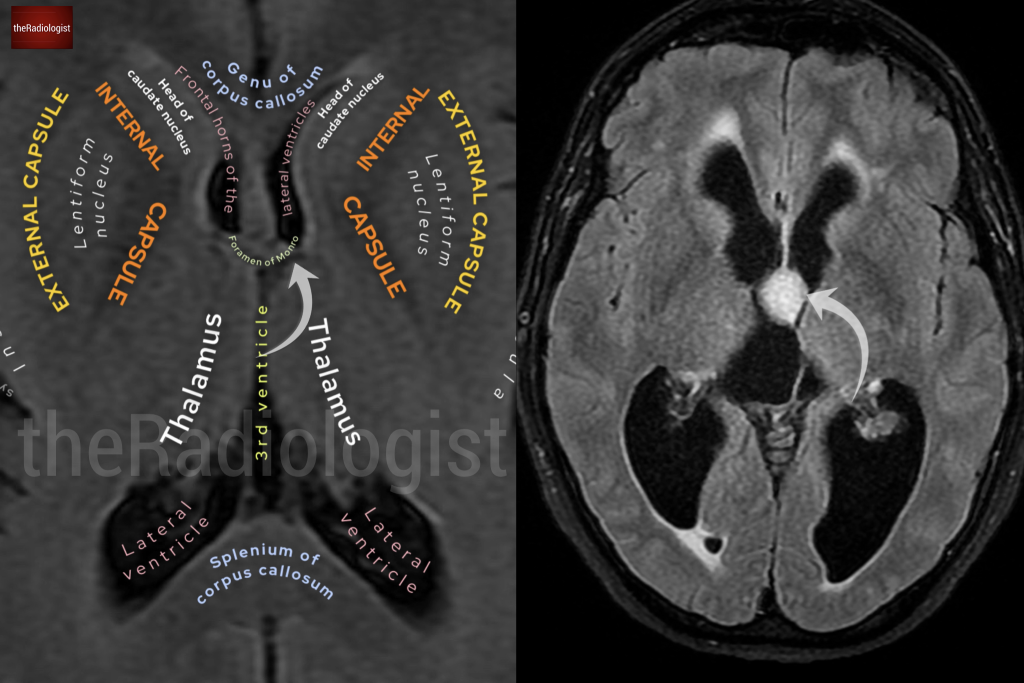
Note the normal anatomy of the foramen of Monro on the left and the presence of an obstructing lesion on the image on the right.
Let’s examine its MRI characteristics:
- FLAIR: The lesion is bright, indicating abnormal tissue.
- T2-weighted: It’s not as bright as CSF but slightly hyperintense compared to grey and white matter.
- T1-weighted: It appears brighter than the surrounding brain tissue.
- Post-contrast images: There is no significant enhancement, ruling out highly vascular lesions.
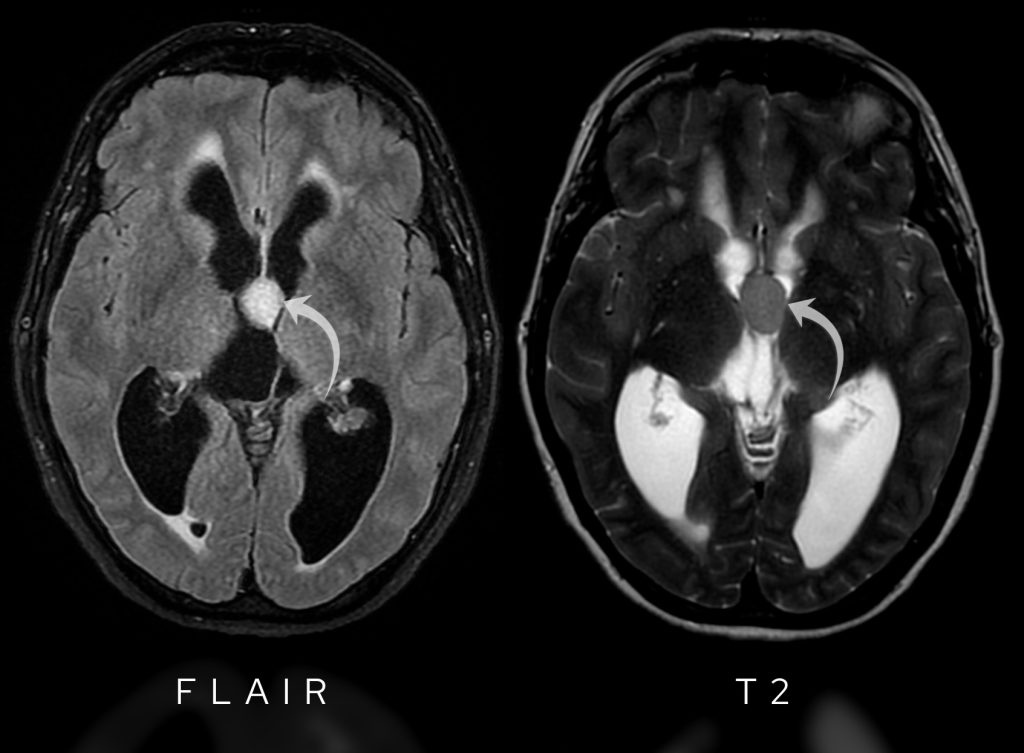
FLAIR images show hyperintensity within the lesion whilst T2-weighted images show the lesion is hypointense to CSF.
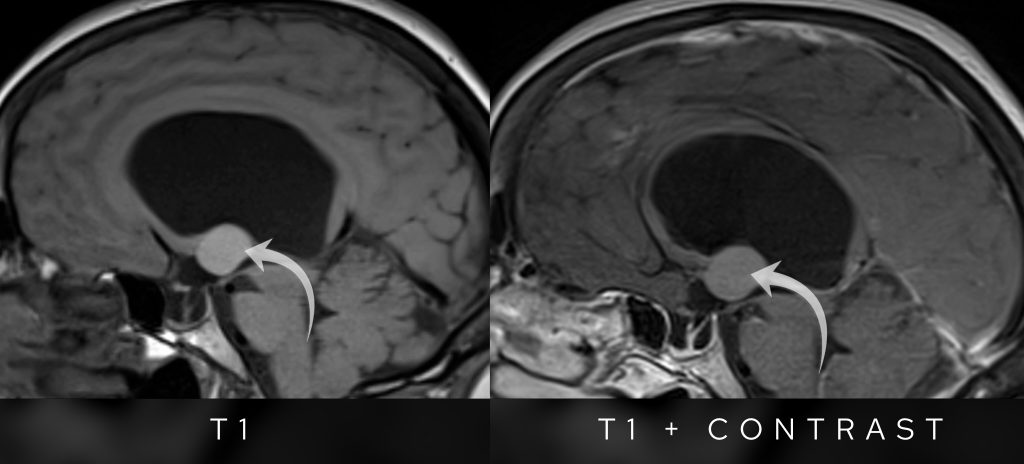
T1 pre and post contrast sagittal images show no appreciable enhancement in the lesion post intravenous gadolinium contrast.
Colloid cyst features
So what is the most likely diagnosis?
The lesion is most compatible with a colloid cyst.
A colloid cyst is a benign epithelial-lined cyst that typically forms at the foramen of Monro. These cysts can be found incidentally on CT scans as small high-density regions in this area.
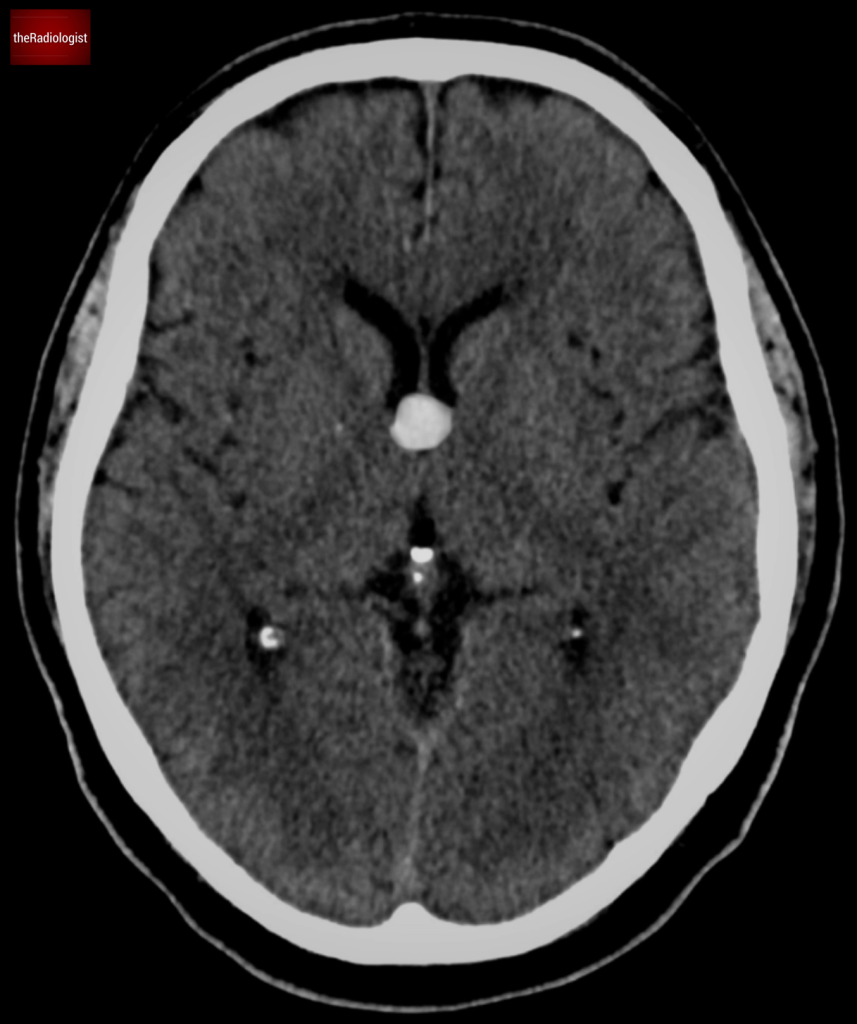
Colloid cysts usually show on CT as a high density lesion in the region of the foramen of Monro.
Why does it matter? Because of its location, even a relatively small colloid cyst can block CSF flow, leading to significant hydrocephalus and symptoms like headache, balance problems, and even sudden neurological decline.
Imaging features
- On non contrast CT look for a well defined hyperdense lesion at the foramen of Monro.
- MRI signal varies depending on the cyst’s fluid content.
- T2 signal intensity decreases if the cyst contains more viscous material, which can make aspiration more difficult.
- Minimal to no contrast enhancement: a helpful feature in differentiating it from other tumors.
Differential
Let’s think about what the differential in this case is.
- Meningioma? No, meningiomas are extra-axial, show strong contrast enhancement, and often have a broad dural base, which is absent here.
- Hemorrhage? The cyst is too well-defined, and its signal pattern doesn’t match typical blood product evolution.
This all points strongly toward a colloid cyst as the leading diagnosis.
Transependymal oedema
Going back to the FLAIR sequence, we see high signal surrounding the lateral ventricles—this is transependymal oedema, an important indicator of acute obstructive hydrocephalus.
What’s happening here?
- The blockage at the foramen of Monro disrupts CSF flow.
- Pressure builds up in the lateral ventricles.
- Fluid leaks into the surrounding brain tissue, causing oedema in the periventricular white matter.
This is a serious finding: it suggests acute hydrocephalus, which, if untreated, can lead to brain herniation and death.
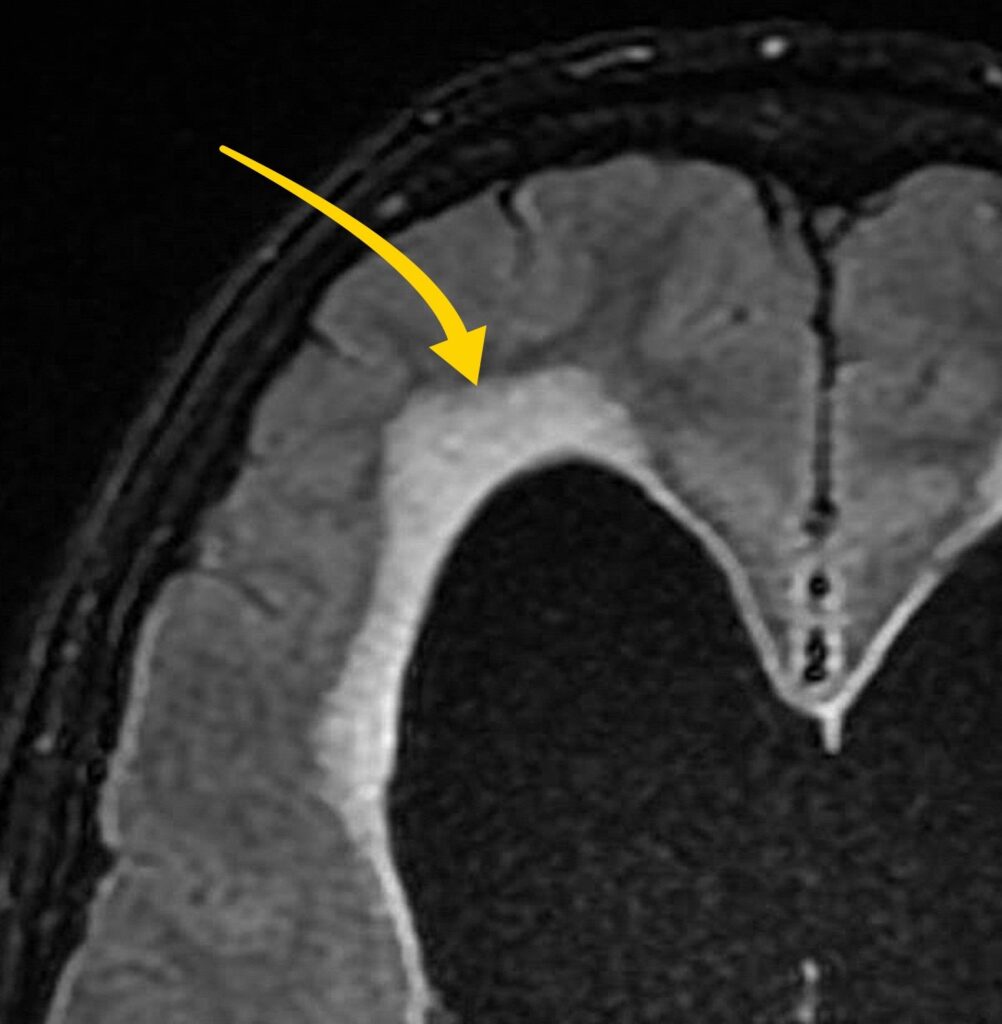
Fluid leak in the context of acute hydrocephalus can lead to transependymal oedema and the appearance of hyperintensity on FLAIR images.
Treatment
The treatment for a colloid cyst depends on:
- Size
- Symptoms
- CSF obstruction
In this case, the colloid cyst was causing life-threatening hydrocephalus, so urgent surgical resection was performed.
Once the cyst was removed, the hydrocephalus resolved, and the patient’s symptoms improved.
Summary
Here’s a summary table of the key features of colloid cysts:
| Colloid cyst facts |
|---|
| Benign cyst filled with gelatinous material |
| Typical location within the anterior third ventricle |
| Variable size |
| Commonly asymptomatic and an incidental finding |
| Can cause acute hydrocephalus/drop attack |
| On CT typically looks bright (hyperdense) |
| MRI can have variable signal characteristics |
KEY POINTS
Don’t forget to overlook the foramen of Monro for a colloid cyst which can be missed.
Transependymal oedema showing as high T2/FLAIR signal on MRI and low density on CT surrounding the ventricles can be a sign of acute hydrocephalus.