Introduction
A 70-year-old man comes in with abdominal pain, and the initial X-ray shows a huge dilated loop of bowel.
This case takes you step by step through how to spot volvulus on plain film, how to tell sigmoid from caecal volvulus, and how to confirm the diagnosis on CT.
You’ll learn what to watch for when assessing for ischaemia or perforation and why recognising this pattern early can make a real difference to patient care.
Case introduction
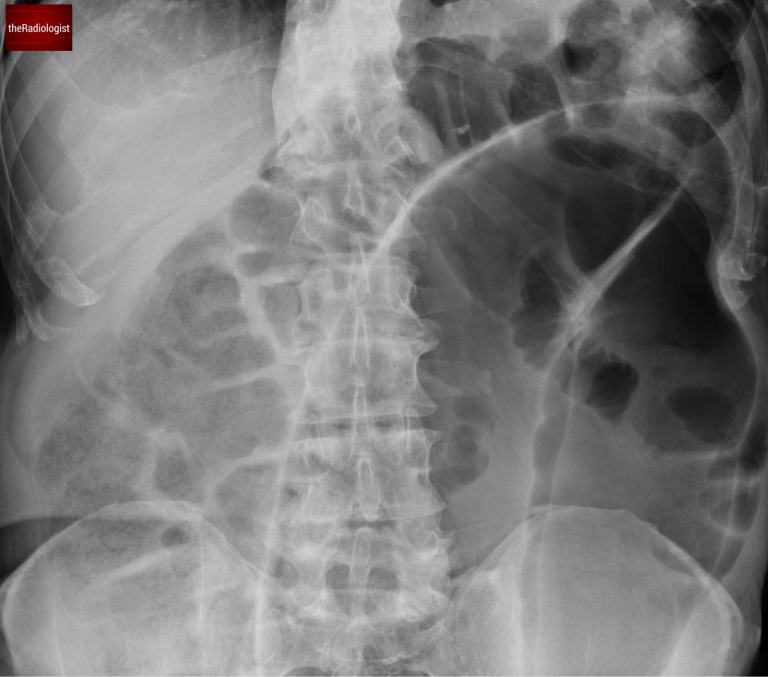
A 70 year old male presents to the Emergency Department with abdominal pain. He has an abdominal X-Ray – have a look at the two images.
Abdominal X-Ray image 1

Abdominal X-Ray image 2
Now have a look through the CT of the abdomen and pelvis. This is post IV contrast in a portovenous phase. I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Video explanation
Here is a video explanation of this case: click full screen in the bottom right corner to make it big. If you prefer though I go through this in the text explanation below.
Abdominal X-Ray review
In the UK at least, abdominal X-Rays are being performed less and less. That is because of their relative insensitivity, their radiation dose and the rise of CT to make a more accurate diagnosis. Nevertheless we have an abdominal film in this case and it is important to still know the basics.
We can see there is a single massively dilated bowel loop – when you see this you need to consider volvulus.
What is volvulus? Volvulus refers to a twisting of the bowel around its mesentery, resulting in obstruction. This condition often occurs in parts of the bowel that are less fixed. Within the colon, the two most common sites for volvulus are the caecum and the sigmoid colon.
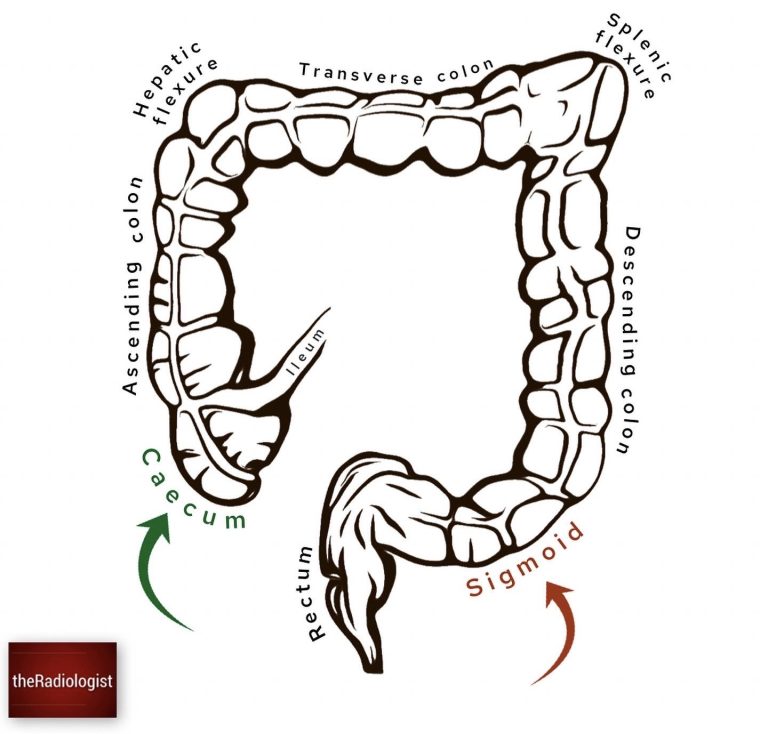
Volvulus most commonly affects the sigmoid colon and caecum given these segments of bowel are less fixed.
Sigmoid versus caecal volvulus
Differentiating between sigmoid and caecal volvulus can be tricky on plain X-rays, but here are some ways to differentiate:
- Age of the Patient:
- Caecal volvulus is more common in younger patients (30–60 years).
- Sigmoid volvulus typically occurs in older patients, like our case.
- Haustral Pattern:
- In caecal volvulus, the haustrae are usually preserved.
- In sigmoid volvulus, you’ll notice loss of the haustral pattern.
- Gas Patterns:
- With caecal volvulus, you might see the left-sided colon collapsed and possibly small bowel dilatation if the ileocaecal valve is patent.
- In sigmoid volvulus, gas may be present in a normal or mildly dilated caecum.
Here is a table outlining the differences:
| Caecal volvulus | Sigmoid volvulus | |
|---|---|---|
| Age | Younger 30-60 | Older |
| Haustral pattern | Preserved | Loss of haustrae |
| Gas pattern | Collapsed left sided colon, possibly small bowel dilatation | Normal caecal gas pattern |
Coffee bean sign
Let’s revisit the first X-ray. The single, dilated bowel loop has a coffee bean appearance—a classic but not entirely specific sign of sigmoid volvulus. The absence of haustra within this loop further supports the diagnosis of sigmoid volvulus.

The massively dilated bowel loop has the appearance of a coffee bean.
Gas pattern
Looking at the second X-ray, there’s a crucial observation: a normal gas pattern within the ascending colon and caecum. This finding is significant because it points us toward sigmoid volvulus – if this was caecal volvulus we wouldn’t be seeing a normal gas pattern within the caecum.
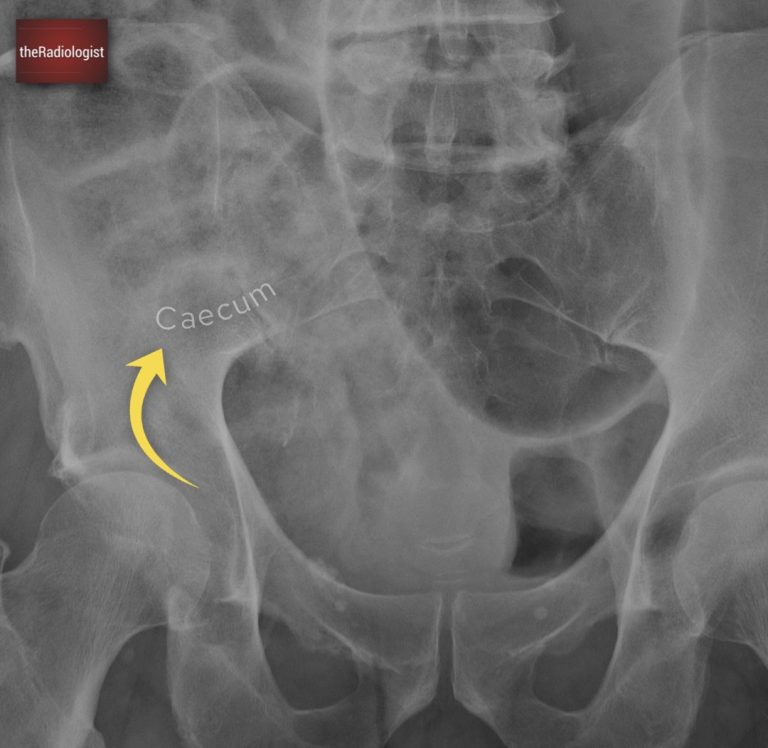
We can see an expected gas pattern within the caecum within the right iliac fossa. If this was caecal volvulus we would not expect to see a normal gas pattern here making sigmoid volvulus more likely.
CT scan review
You’ve seen the axial slices but below I’ve shown coronal slices of the same CT, here’s what we see:
- The rectum, positioned normally in the pelvis.
- Free fluid in the pelvis, lateral to the rectum.
- Following the bowel, there’s a whirling appearance in the sigmoid colon, consistent with the site of torsion.
- A dilated bowel loop proximal to the whirl sign.
This is a textbook case of sigmoid volvulus. Now you’ve seen this review for ischaemia by looking for gas within the bowel wall and lack of enhancement whilst check lung windows to make sure there is no extraluminal gas representing a perforation.
Follow the rectum through – you will first see a whirl within the sigmoid before finding dilated obstructed sigmoid proximal to this, accounting for the X-Ray finding.
Treatment
The initial treatment for sigmoid volvulus is typically endoscopic decompression, which can relieve the obstruction.
While CT scans are increasingly the go-to tool for diagnosing conditions like sigmoid volvulus, radiologists must still be adept at interpreting X-rays. Recognizing the features of volvulus on X-rays can make a life-saving difference, especially in settings where CT may not be immediately available.
KEY POINT
Once you see a ‘coffee bean’ sign on X-Ray, consider sigmoid volvulus.
Think about the patient demographic and look for gas within the caecum and ascending colon which can help differentiate sigmoid from caecal volvulus.
Free guide: 20 Chest X-Ray signs you need to recognise
Downloaded by 10,000+ healthcare professionals.
Get 20 annotated chest X-ray signs with clear teaching points and explanations. Written by a Consultant Radiologist, this free guide is designed to help you recognise important findings more confidently when reviewing chest X-Rays.