A male in his 50s has a CT of his abdomen and pelvis which reveals areas of low attenuation that need closer assessment. This case covers how to identify the contrast phase, distinguish infarction from pyelonephritis, and think through potential causes.
A male in his 50s presents with upper abdominal pain and has a CT abdomen and pelvis with IV contrast.
Have a look at the scan below.
I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Assess the contrast phase
Let’s start by having a look at the spleen. When assessing the spleen on a post contrast CT it is important to firstly assess which phase of contrast we are currently in. That is because on an arterial phase CT the spleen can appear very heterogeneous due to variable contrast flow rates through the open and closed circulation. This can easily be confused for pathology but is in fact normal!
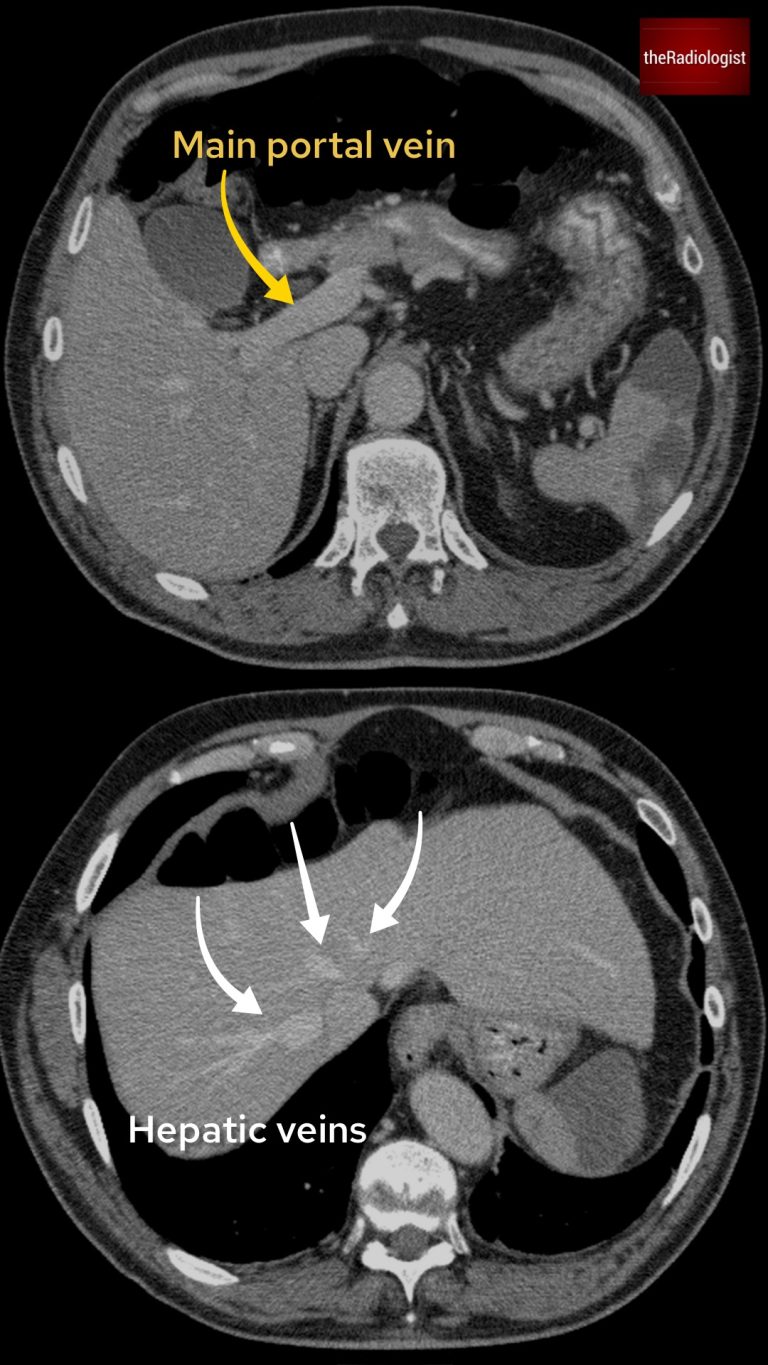
In this case we are in what is called a ‘portal venous phase’: we can see from the images below that both the main portal vein and the hepatic veins are well opacified. This means we are not in an arterial phase and we can reliably assess the spleen.
If you can see the main portal vein and hepatic veins opacified then you can say the scan has been performed in a portal venous phase (usually 70-90 seconds post intravenous contrast injection).
Now the spleen does not appear normal – there are wedge shaped regions of low density seen throughout the spleen. With anything ‘wedge shaped’ the first thing to think about is a vascular cause and infarction.
Low density wedge shaped regions within the spleen. With anything wedge shaped always consider infarction.
Assessing the kidneys
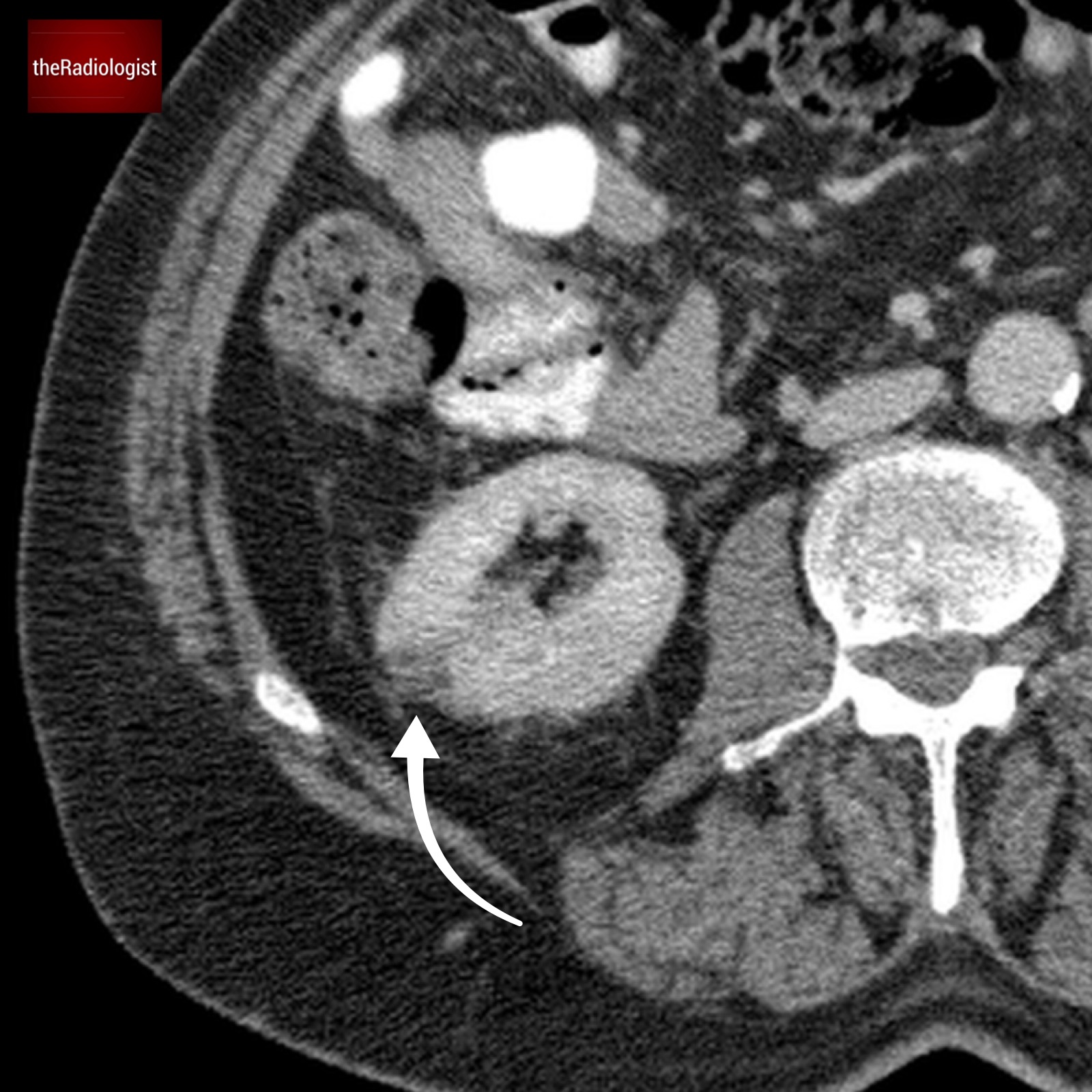
Don’t stop there – have a look at the kidneys and in amongst some simple cysts and renal cortical scarring you will find a similar pattern of wedge shaped low density. With wedge shaped regions within the kidneys, it can be tricky to assess the cause as infarction and pyelonephritis can have similar appearances both causing wedge shaped regions of low density.
The ‘cortical rim sign’ can sometimes be seen in infarction where at the periphery of the wedge of low density there is a shallow rim of normal appearing renal cortex. This region is supplied by perforating branches of the renal capsular artery. If this sign is present you can say the cause is infarction but unfortunately if it is not present you are no further forward as it is not always present in infarction.
In our case there is no cortical rim sign – we can see low density extending all the way out to the periphery. In radiology there are often times where two things can have identical appearances but it is about putting the whole picture together be it the clinical picture or the other features of the scan. In this case the fact you have splenic infarcts makes it most likely that the pathology affecting the kidneys is also infarction rather than pyelonephritis.
Wedge shaped region of low density within the right kidney the differential of which is between pyelonephritis and infarction. ‘Cortical rim sign’ not present.
DIAGNOSIS
The CT findings are consistent with both splenic and renal infarction.
Cause of infarction
Atrial fibrillation and subsequent thromboembolism is a common cause of acute renal and splenic infarction and should be investigated for even in the presence of a normal ECG. Other potential causes include septic emboli and a prothombotic state related to malignancy. An Echo is usually good idea to assess for a cardioembolic source and check the valves for endocarditis.
KEY POINTS
When assessing the spleen on a post contrast CT it is important to check the phase of imaging as the spleen can appear spuriously abnormal on arterial phase CT.
FREE GUIDE
Free guide: 20 Chest X-Ray signs you need to recognise
Downloaded by 10,000+ healthcare professionals. Get 20 annotated chest X-ray signs with clear teaching points and explanations. Written by a Consultant Radiologist, this free guide is designed to help you recognise important findings more confidently when reviewing chest X-Rays.
You’ve got the framework now let’s put it to work. Dive into a related case to see these findings on real images, or explore another guide to build out your systematic approach. That’s where it really starts to stick.