Small bowel obstruction
Dilated bowel loops and key review areas on CT and X-Ray
Introduction
A woman in her 60s presents with lower abdominal pain. She has an X-Ray and then an abdominal CT. Her CT scan shows features suggesting small bowel obstruction.
In this case, we review the CT and X-ray findings, go over how to distinguish small from large bowel obstruction, explore possible causes, and discuss next steps in management.
Case introduction
A female in her 60s presents with abdominal pain. There is a history of previous abdominal surgery, diabetes mellitus type II and atrial fibrillation. Have a look at the abdominal X-Ray below.

Abdominal X-Ray on presentation
CT scan
Now have a look through the CT of the abdomen and pelvis. This is post IV contrast in a portovenous phase. I know you want to get going but you may need to wait a few seconds for the scan to load. Tap the first icon on the left to scroll.
Approaching dilated bowel loops
In the UK at least, abdominal X-Rays are being performed less and less. That is because of their relative insensitivity, their radiation dose and the rise of CT to make a more accurate diagnosis. Nevertheless we have an abdominal film in this case and it is important to still know the basics.
We can see some prominent bowel loops in the centre of this film suggesting there may be bowel obstruction. How can we tell the difference between small and large bowel obstruction?
| Small | Large | |
|---|---|---|
| Diameter of bowel loops when obstructed | >3 cm | >5 cm (>9 cm if caecum) |
| Indentations seen | Valvulae conniventes (traverse whole bowel wall) | Haustrae (just periphery) |
| Location | Central | Peripheral |
Firstly if you see very dilated bowel loops it is unlikely you are dealing with small bowel as this would perforate before it gets to a diameter of 5 cm. The easiest way to tell if you are dealing with small or large bowel dilatation is to look at the indentations on the bowel wall.
With small bowel you have valvulae conniventes which traverse the whole bowel. In comparison with large bowel you have haustrae only seen at the periphery.
Also look at the location – small bowel loops will more likely live centrally whilst large bowel has a more peripheral location.
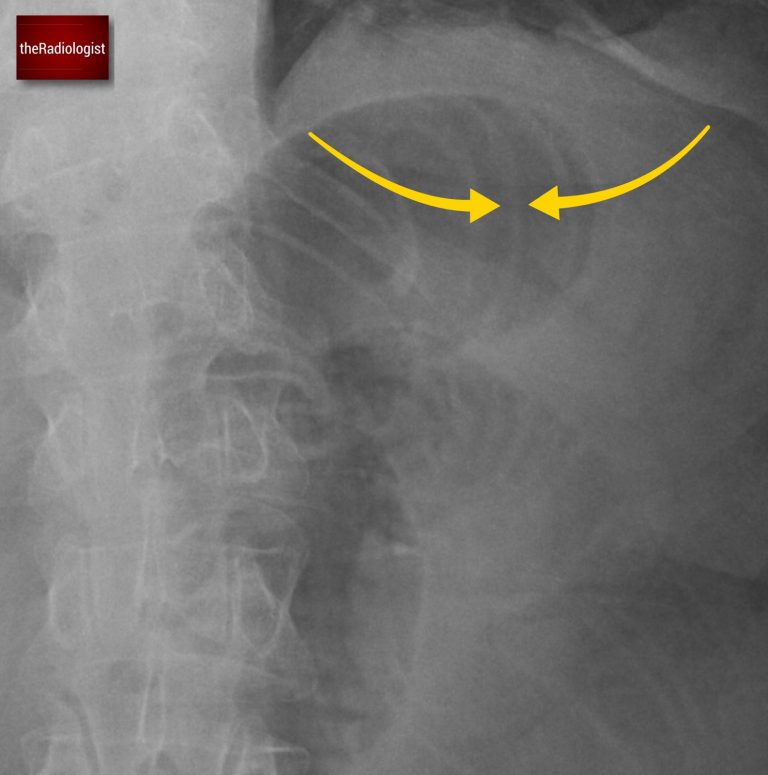
Look at the indentations on the bowel wall. With small bowel look out for valvulae conniventes (yellow arrow) that traverse the whole bowel wall: we can see this here, this is small bowel dilatation.
CT scan findings
Now let’s look at the CT scan. I like to follow the large bowel from the rectum and follow it up. If you do so in this case you will find the whole of the large bowel is not dilated and normal in calibre, essentially excluding large bowel obstruction.
Go to the bottom of the scan and find the rectum then follow the colon all the way round.
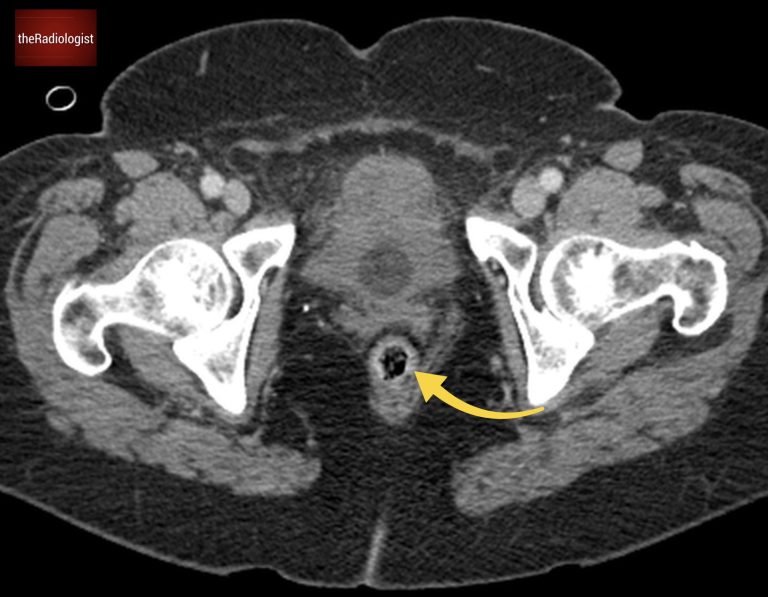
Now looking elsewhere we can see fluid filled dilated bowel loops – these are small bowel loops. There are however other loops of small bowel which are not dilated. This implies mechanical small bowel obstruction – here we are looking for dilated small bowel proximal to collapsed small bowel with a sharp transition point between the two.
It is now a case of following the small bowel and looking for a transition point between dilated and collapsed small bowel. I like to start from the stomach and follow the small bowel round. If you do so eventually you will come across a transition point within the right side of the abdomen from dilated small bowel to collapsed small bowel.
Find this small bowel loop on the right side of the abdomen. Once you follow this you will find it leads to a transition point where distal to this there are only collapsed small bowel loops.
Causes of small bowel obstruction
The two most common causes of small bowel obstruction are:
- Adhesional small bowel obstruction (with a history of previous abdominal surgery)
- Hernias
The former is the most likely scenario here. This can usually be treated conservatively in the first instance, unlike a hernia which will usually need reduction and surgical repair to relieve the small bowel obstruction. In bowel ischaemia you may find dilated bowel loops only as an early sign but there won’t usually be a sharp transition point to dilated bowel loops like you have here.
Let’s have a more comprehensive look at causes of small bowel obstruction in the table below:
| Cause | Notes |
|---|---|
| Adhesions | Most common cause. Usually post-operative so put any surgical history on your CT abdomen pelvis request! |
| Hernia | Can be more commonly an external hernia eg inguinal, femoral, abdominal wall. But can also be an internal hernia. |
| Tumour | Small bowel tumours are no where near as common as large bowel tumours. External compression from peritoneal disease or nodes also possible. |
| Crohn’s disease | Inflammatory strictures or adhesions can cause small bowel obstruction. Terminal ileum a commonly affected location. |
| Volvulus | Small bowel twisting on itself. May be associated with congenital malrotation. |
| Intussusception | More common in children. In adults usually has a lead point such as underlying polyp or tumour. |
| Gallstone ileus | A gallstone erodes through the gallbladder into bowel and obstructs the small bowel. Classic exam question – look for gas within the biliary tree (usually central unlike portovenous gas which is peripheral within the liver). |
| Radiation enteritis | Fibrosis and strictures secondary to previous radiotherapy. |
| Foreign body | Including bezoars. |
| Congenital causes | Such as atresia, stenosis and malrotation. |
KEY POINTS
It can be tedious but once you see dilated bowel loops on a CT you need to follow the bowel round looking for a transition point.
In mechanical bowel obstruction you are looking for dilated bowel loops with a sharp transition to collapsed bowel loops. The exception is closed loop obstruction where you will two transition points – one from collapsed to dilated then again from dilated to collapsed.
Diffusely dilated bowel without transition could represent ‘pseudo-obstruction’ or ‘ileus’, causes of which include post-operative state, electrolyte imbalances and drugs.
Free guide: 20 Chest X-Ray signs you need to recognise
Downloaded by 10,000+ healthcare professionals.
Get 20 annotated chest X-ray signs with clear teaching points and explanations. Written by a Consultant Radiologist, this free guide is designed to help you recognise important findings more confidently when reviewing chest X-Rays.